In severe aortic stenosis with intermediate surgical risk, TAVR was noninferior to SAVR for death or disabling stroke
- Spencer, Frederick A. MD
- Guyatt, Gordon H. MD
Question
In patients with severe symptomatic aortic stenosis and intermediate surgical risk, is transcatheter aortic valve replacement (TAVR) noninferior to surgical aortic valve replacement (SAVR)?
Methods
Design
Randomized, controlled, noninferiority trial (Surgical Replacement and Transcatheter Aortic Valve Implantation [SURTAVI] trial). ClinicalTrials.gov NCT01586910.
Allocation
Concealed.
Blinding
Unblinded.
Follow-up period
2 years.
Setting
87 centers in the USA, Europe, and Canada.
Patients
1746 patients (mean age 80 y, 57% men) who had symptomatic, severe aortic stenosis and intermediate surgical risk (estimated 30-d risk for surgical death 3% to 15% based on Society of Thoracic Surgeons Predicted Risk of Mortality and coexisting illnesses, frailty, and disability).
Intervention
TAVR with a self-expanding bioprosthesis (n = 879) or SAVR (n = 867).
Outcomes
Primary outcome was a composite of all-cause mortality or disabling stroke (based on Valve Academic Research Consortium-2 criteria) at 2 years. Secondary outcomes included components of the primary outcome, complications related to the procedures, cardiovascular outcomes, and quality of life.
Patient follow-up
95% (modified intention-to-treat analysis).
Main results
The main results are in the Table. Quality of life did not differ between groups at 1 year.
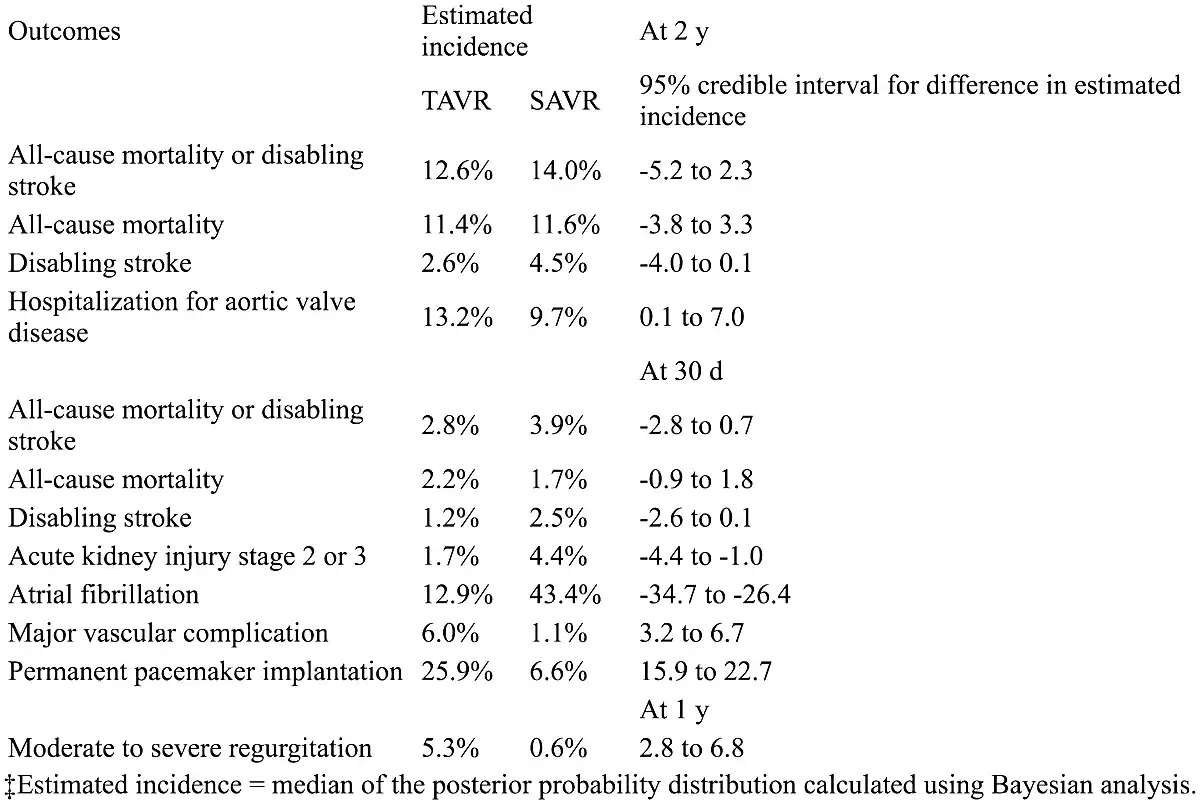
Conclusions
In patients with severe aortic stenosis and intermediate surgical risk, transcatheter aortic valve replacement (TAVR) was noninferior to surgical replacement for mortality and disabling stroke. Surgery increased short-term acute kidney injury and atrial fibrillation. TAVR increased short-term pacemaker implantation and major vascular complications and long-term hospitalization for aortic disease and regurgitation.