Review: In VTE, reduced- and full-dose extended DOAC therapies do not differ and are better than no extended therapy
- DeLoughery, Thomas MACP, FAWM
Question
In patients with venous thromboembolism (VTE) treated with anticoagulants for up to 1 year, what are the efficacy and safety of extended treatment with reduced-dose, direct oral anticoagulants (DOACs) compared with full-dose DOACs or no anticoagulation?
Review scope
Included studies compared extended-duration, reduced-dose DOACs with full-dose DOACs or no anticoagulation in adults ≥ 18 years of age with VTE (deep venous thrombosis or pulmonary embolism) who had received acute anticoagulant treatment for 3 to 12 months and for whom stopping anticoagulant treatment could be considered, and reported recurrent VTE and bleeding events. Studies of anticoagulants not approved for VTE treatment were excluded.
Review methods
MEDLINE, EMBASE/Excerpta Medica, CINAHL (to Apr 2017); conference abstracts from the International Society on Thrombosis and Haemostasis and American Society of Hematology; and reference lists were searched for randomized controlled trials (RCTs). 2 RCTs (n = 5847) (mean age 58 y) met the selection criteria. The reduced- and full-dose DOACs were apixaban (2.5 mg and 5 mg, twice daily) in 1 trial and rivaroxaban (10 mg and 20 mg, once daily) in the other. Each drug was administered for 12 months in extended treatment. No-anticoagulant controls were placebo and aspirin, 81 mg once daily. Follow-up was at 1 year. Both trials adequately reported randomization sequence generation, allocation concealment, blinding of patients and personnel, and blinding of outcome assessors.
Main results
The main outcomes are in the Table.
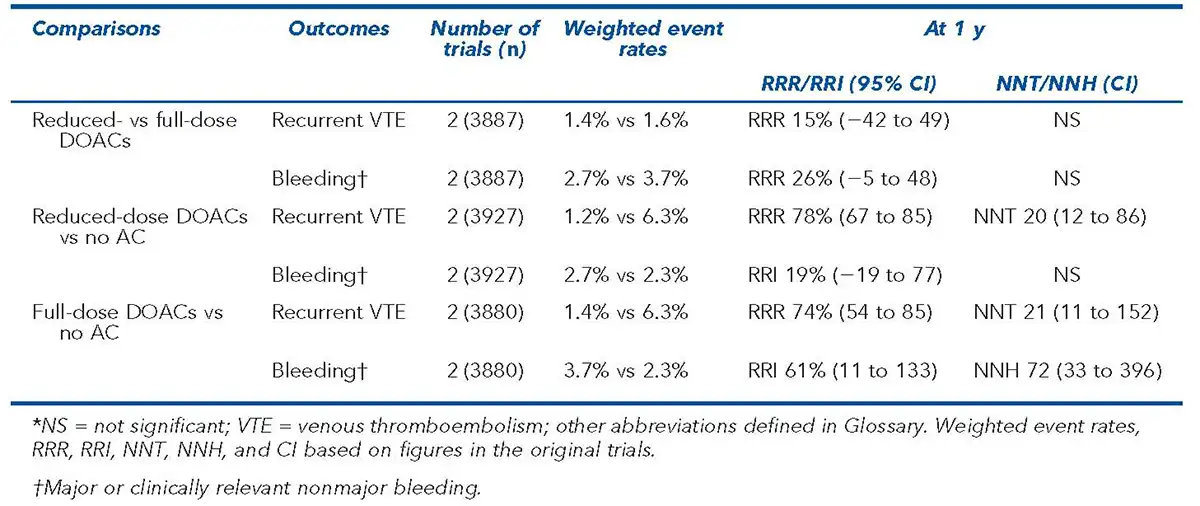
Conclusions
In patients with venous thromboembolism (VTE) treated with anticoagulants for up to 12 months, extended-duration, reduced-dose direct oral anticoagulants (DOACs) did not differ from full-dose DOACs for recurrent VTE or bleeding. Reduced-dose DOACs decreased recurrent VTE more than placebo or aspirin without increasing risk for bleeding.