Coronary CTA reduced risk for coronary events at 5 years in patients with stable chest pain
- Hudson, Michael P. MD
Question
In patients with stable chest pain, does adding coronary computed tomographic angiography (CTA) to usual care reduce adverse coronary outcomes at 5 years?
Methods
Design
Long-term follow-up of a randomized controlled trial (RCT) (Scottish Computed Tomography of the Heart [SCOT-HEART] trial). ClinicalTrials.gov NCT01149590.
Allocation
Concealed.
Blinding
Unblinded.
Follow-up period
Median 4.8 years.
Setting
12 outpatient cardiology clinics in Scotland, UK.
Patients
4146 adults 18 to 75 years of age (mean age 57 y, 56% men) who were referred to the cardiology clinic by a primary care physician for stable chest pain. Exclusion criteria included severe renal failure, major allergy to iodinated contrast agent, or acute coronary syndrome in the past 3 months.
Intervention
Usual care plus coronary CTA (n = 2073) or usual care alone (n = 2073). All patients were managed at the discretion of the physician. For patients in the CTA group, physicians were prompted to consider the CTA results in their management decisions; for patients in the usual care group, physicians were prompted to consider the results of the ASSIGN cardiovascular risk score in their management decisions. Physicians were encouraged to prescribe preventive therapies if there was nonobstructive or obstructive coronary heart disease (CHD) on the CTA or the patient's ASSIGN score was ≥ 20.
Outcomes
Primary outcome was a composite of death from CHD or nonfatal myocardial infarction (MI). Secondary outcomes included a composite of death from CHD, nonfatal MI, or nonfatal stroke; all-cause mortality; individual components of the primary and secondary composite outcomes; and rates of invasive coronary angiography and revascularization.
Patient follow-up
98% for the primary 5-year outcome (intention-to-treat analysis).
Main results
The main results are in the Table.
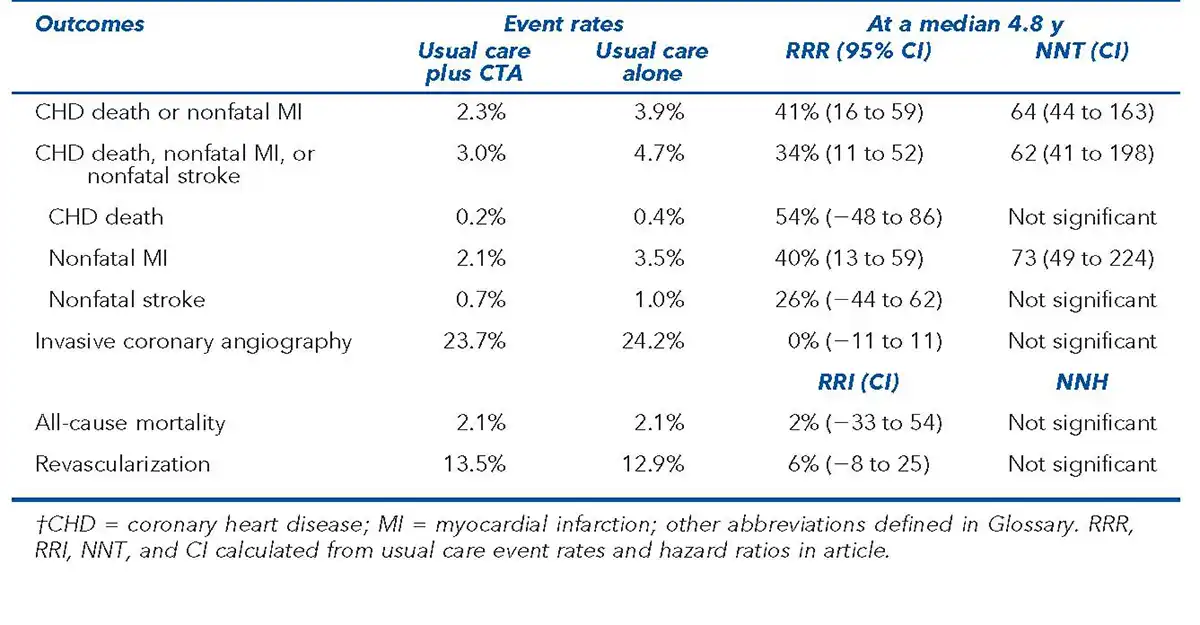
Conclusion
In patients with stable chest pain, adding coronary computed tomographic angiography to usual care reduced 5-year risk for coronary outcomes, primarily through reduction of nonfatal MI.