Botulinum toxin type A (BTX-A) is widely employed in the treatment of facial rhytids, facial asymmetry, and hyperhidrosis. Its pathophysiology involves presynaptic inhibition of acetylcholine release at neuromuscular junctions, causing targeted muscle paralysis. Its ease of use, efficacy, and excellent safety profile make it a popular treatment option in aesthetic practice.
Laser therapy is another widely utilized treatment modality in aesthetic practice, with proven benefit in treating facial rhytids, scars, and skin resurfacing. A variety of lasers are utilized, each targeting particular chromophores such as melanin, water, and hemoglobin, using specific wavelengths of collimated light to induce thermal, chemical, or mechanical changes in the respective tissue. Lasers can be ablative, removing the epidermis and heating the dermis to stimulate collagen formation, as with carbon dioxide (CO2) and erbium lasers, or nonablative lasers, which are less aggressive and do not remove the epidermis, as with pulsed dye, Erbium:YAG lasers, and intense pulsed light (IPL). Both ablative and nonablative lasers can be fractionated, producing microscopic columns of unaffected tissue within the treatment zone to accelerate recovery and minimize local side effects. There is evidence to suggest that routine adjunctive use of botulinum A toxin and laser therapy is more efficacious, and safer, than a single treatment alone (Table 1).
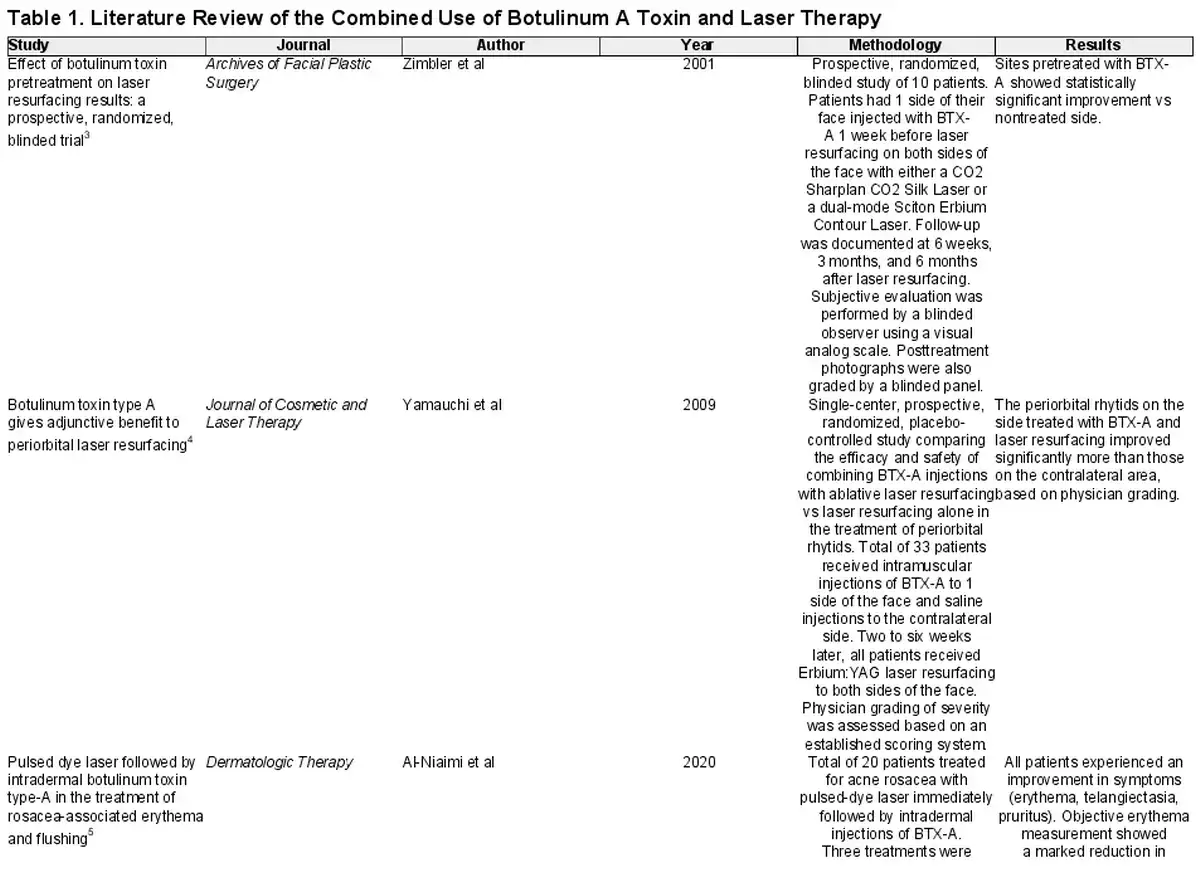
Zimbler et al's randomized blinded study reported a statistically significant improvement in facial rhytids at the different subsites that were treated with botulinum toxin injections followed by ablative laser therapy, compared to those treated with ablative laser therapy alone (P ≤ .05). The brands of laser included the Sharplan CO2 Silk Laser (ECS Sharplan Corp., Norwood, MA; λ = 10,600 nm) and the dual-mode Sciton Erbium Contour Laser (Sciton, Palo Alto, CA; λ = 2940 nm), with the choice of laser dependent on patient preference and Fitzpatrick skin type. This improvement in facial rhytids was sustained at the 6 month follow-up, with facial rhytids at the crow's feet subsite showing the most improvement. In a randomized, placebo-controlled study Yamauchi et al also found that periorbital rhytids treated with botulinum toxin and laser resurfacing showed more improvement compared to periorbital rhytids treated with laser resurfacing alone. The combination of BTX-A and adjunctive laser therapy has also been reported to improve the appearance of acne rosacea, with respect to the erythema, telangiectasias, and pruritus experienced by patients.
Both ablative as well as nonablative laser therapies were considered in the studies. Yamauchi et al employed ablative laser resurfacing with Erbium:YAG (NaturaLase, Bethel, CT; λ = 1064, 532, 585, 650 nm); Zimbler et al utilized the Sharplan CO2 Silk Laser and a dual-mode erbium contour laser (Sciton Erbium Contour Laser); and Mahmoud et al used the Ultra-Pulse fractional ablative carbon dioxide laser (Lumenis Aesthetic, San Jose, CA; λ = 10,600 nm).,, Al-Niaimi et al employed a pulsed-dye laser (Vbeam, Candela, MA; λ = 595 nm), and patients in Fan et al's study were treated with nonablative fractional laser therapy (Crown of the King, Lumenis; λ = 1565 nm)., The dose of botulinum A toxin also varied, ranging from 5 to 50 units, depending on the route of delivery and the brand of BTX-A. Patients in the study conducted by Al-Niaimi et al also received varying doses of BTX-A depending on the extent and severity of their symptoms.
In two studies the topical form of BTX-A was utilized instead of the injected form., Fan et al gave the risks associated with subcutaneous botulinum injections to the upper and lower eyelids as reason to assess the efficacy of topical BTX-A in treating facial rhytids in this region. The authors of the study demonstrated an improvement in the appearance of periocular wrinkles when topical BTX-A was provided in addition to nonablative laser resurfacing. Mahmoud et al reported that topical BTX-A alone was ineffective in treating facial rhytids, which led the authors to investigate whether using topical BTX-A as an adjunct with laser therapy improved its efficacy. The authors confirmed a more positive outcome with topical BTX-A as adjuvant therapy to ablative laser resurfacing.
In both the randomized studies conducted by Yamauchi et al and Zimbler et al, ablative laser therapy was performed after treatment with BTX-A injections. In the study by Yamauchi et al, laser therapy was performed 2 to 6 weeks following injections with BTX-A, and in Zimbler et al's study laser therapy was performed 1 week after BTX-A., There has often been uncertainty surrounding the order and temporality of BTX-A and laser therapy given in combination. One view is that laser therapy should be carried out before treatment with BTX-A because of concerns regarding deactivation of the botulinum toxin or diffusion of the BTX-A molecules by the laser, but there is little literature to support one way or the other.
Semchyshyn and Kilmer conducted a prospective study to investigate whether nonablative laser therapy inactivated botulinum toxin in the treatment of facial rhytids. The following lasers were included in the study: VBeam (Candela), SmoothBeam (Candela; λ = 1450 nm), Quantum IPL (Lumenis; λ = 560–1200 nm), CoolGlide (Cutera, Brisbane, CA; λ = 1064 nm), and the radiofrequency device ThermaCool TC (Solta Medical, Bothell, WA). No decrease in botulinum toxin efficacy was found when patients were treated with laser therapy immediately after BTX-A was injected compared to when laser therapy was performed before BTX-A was injected. Moreover, no other unwanted effects such as muscle paralysis to surrounding muscles occurred as a result of performing laser therapy immediately after BTX-A.
There is some support in the literature for the safe, concomitant use of botulinum toxin A and ablative or nonablative lasers in facial aesthetic practice, with the suggestion that combined use may be of more benefit than a single agent alone. Our report is limited to the limited availability of evidence. Although high-level studies such as prospective randomized control trials have been performed, and their data are included in this report, the patient numbers are too low for the conclusions to be entirely robust. In our experience, combination treatment is practical and safe. The lack of evidence regarding the temporality or order of treatments leaves the decision dependent on patient sensitivity, finances, clinic capacity, and regularity of follow-up. In our practice, we decide which agent to provide based on the patient's most pressing concerns, often with BTX-A treatment carried out first with a patch test, followed by laser therapy 1 week later. For regular patients, we opt for BTX-A injection before immediate laser treatment to minimize discomfort of BTX-A injection into more sensitive skin following laser treatment.
REFERENCES
- 1. Patil UA, Dhami LD. Overview of lasers. Indian J Plast Surg. 2008;41(Suppl):S101–S113. doi:
- 2. Preissig J, Hamilton K, Markus R. Current laser resurfacing technologies: a review that delves beneath the surface. Semin Plast Surg. 2012;26(3):109–116. doi:
- 3. Zimbler MS, Holds JB, Kokoska MS, et al Effect of botulinum toxin pretreatment on laser resurfacing results: a prospective, randomized, blinded trial. Arch Facial Plast Surg. 2001;3(3):165–169. doi:
- 4. Yamauchi PS, Lask G, Lowe NJ. Botulinum toxin type A gives adjunctive benefit to periorbital laser resurfacing. J Cosmet Laser Ther. 2004;6(3):145–148. doi:
- 5. Al-Niaimi F, Glagoleva E, Araviiskaia E. Pulsed dye laser followed by intradermal botulinum toxin type-A in the treatment of rosacea-associated erythema and flushing. Dermatol Ther. 2020;33(6):e13976. doi:
- 6. Mahmoud BH, Burnett C, Ozog D. Prospective randomized controlled study to determine the effect of topical application of botulinum toxin A for crow's feet after treatment with ablative fractional CO2 laser. Dermatol Surg. 2015;41(Suppl 1):S75–S81. doi:
- 7. Fan X, Yin Y, Wang S, et al Clinical assessment of the safety and effectiveness of nonablative fractional laser combined with transdermal delivery of botulinum toxin A in treating periocular wrinkles. Plast Reconstr Surg Glob Open. 2016;4(8):e1004. doi:
- 8. Semchyshyn NL, Kilmer SL. Does laser inactivate botulinum toxin?Dermatol Surg. 2005;31(4):399–404. doi: