Introduction
Renin-angiotensin-aldosterone system inhibitors (RAASis) are the cornerstone for managing patients with chronic kidney disease (CKD). The clinical benefits of RAASis have been well established in both renal and cardiovascular diseases [–], reducing both the progression of kidney disease and the risk of end-stage renal disease [, , ], as well as improving cardiovascular outcomes including reduced risk of hospitalization with heart failure (HF) [], myocardial infarction, stroke, and cardiovascular death [], and all-cause mortality [].
Patients with CKD are at increased risk of hyperkalaemia due to dysregulation of potassium (K+) homoeostasis following a reduction in kidney function [, ]. Increased risk of hyperkalaemia also occurs in patients with HF, or both HF and CKD [, ], and is further increased by comorbid insulin resistance [] or RAASi use [, ]. Importantly, hyperkalaemia is associated with increased hospitalizations, all-cause and cardiovascular mortality, peripheral neuropathy, and renal tubular acidosis [], with mortality rates as high as one-third reported in patients with severe hyperkalaemia (serum K+ [sK+] ≥6.5 mEq/L) [] or in hyperkalaemic patients with combined CKD, HF, and type 2 diabetes mellitus (T2DM) []. Hyperkalaemia often leads to RAASi dose reduction or discontinuation [1, 3, 5, 16]. A large US database study found that RAASi dose was reduced from optimal levels, or stopped entirely, 47% of the time following moderate-to-severe hyperkalaemic events [], this being associated with a two-fold increase in mortality and worse cardio-renal outcomes compared with patients on optimal RAASi []. For this reason, the Kidney Disease Improving Global Outcomes (KDIGO) Guidelines recommend RAASi dose reduction or discontinuation in hyperkalaemic patients as a final resort only, following failure of all other therapeutic options to lower sK+ []. It is recognized that once stopped, RAASis are frequently never restarted despite ongoing clinical need.
Patiromer is an oral non-absorbed calcium-exchange potassium binder, which acts to bind potassium ions in the gastrointestinal tract, leading to potassium excretion in faeces []. In patients with hyperkalaemia, long-term patiromer has been shown to reduce sK+ and enable optimum RAASi therapy in numerous clinical trials [–], with evidence of long-term efficacy and safety up to 12 months [, ]. The ability of patiromer to reduce serum aldosterone levels, blood pressure (BP), and albumin-to-creatinine ratio in hyperkalaemic patients has also been reported, although less extensively [, ].
The overall aim of this study was to assess the impact of patiromer on the continuation of RAASi therapy in patients with CKD and T2DM enrolled in the AMETHYST-DN trial (hereafter referred to as AMETHYST), compared with a propensity score-matched, real-world cohort of patients not receiving patiromer from the Salford Kidney Study. The impact of RAASi enablement with patiromer on proteinuria and BP was studied as a secondary aim.
Materials and Methods
AMETHYST methods have been described previously []. Briefly, AMETHYST (NCT01371747) was a multicentre, phase 2, open-label trial of patiromer in 304 adult patients on RAASi with CKD (estimated glomerular filtration rate [eGFR] 15–<60 mL/min/1.73 m2), T2DM, hyperkalaemia (sK+ >5.0 mEq/L), and hypertension (average systolic BP >130 to ≤180 mm Hg and diastolic BP >80 to ≤110 mm Hg). Patients were randomized to patiromer 8.4–33.6 g/day, depending on baseline hyperkalaemia stratification, for an 8-week treatment phase followed by a 44-week maintenance phase. Patiromer was titrated throughout the trial period as needed to reach and maintain serum K+ ≤5.0 mEq/L. The protocol was approved by local or national independent ethics committees at each study site.
Detailed methods of the Salford Kidney Study are also published elsewhere []. In brief, the Salford Kidney Study is a prospective observational cohort of non-dialysis CKD patients in Salford, Greater Manchester, UK. Starting in 2002, the study has recruited adult patients with CKD (eGFR <60 mL/min/1.73 m2), who were able to provide informed consent and were referred to the renal services at Salford Royal Hospital, in the Northern Care Alliance NHS Foundation Trust.
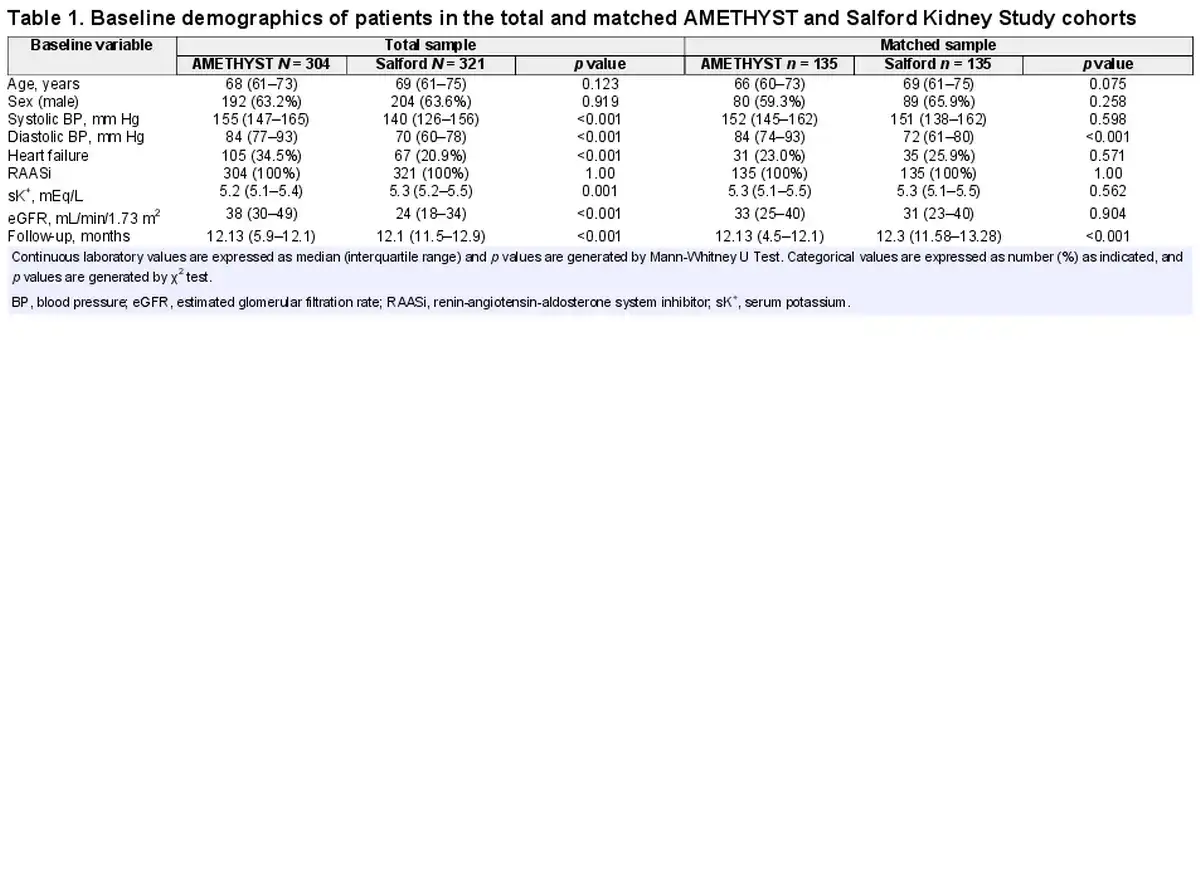
From the 3,564 patients recruited into the Salford Kidney Study, 321 patients of white ethnicity with CKD, T2DM, hyperkalaemia, and receiving RAASi underwent propensity score matching with the 304 AMETHYST patients (online suppl. Fig. 1; for all online suppl. material, see https://doi.org/10.1159/000533753). Matching was performed for systolic BP, HF status, and eGFR at baseline by propensity scores generated from a logistic regression analysis (1:1, nearest neighbour method, calliper distance 0.2) (Table 1). All patients were followed up for a minimum duration of 12 months after hyperkalaemia detection (Table 1). The median change in sK+, urine albumin-to-creatine ratio (uACR), eGFR, and BP over the 12-month follow-up was calculated by subtracting the data for each individual patient at 12 months from the baseline value for this individual then calculating median interquartile range (IQR) for each group. p values comparing the change from baseline in AMETHYST and the Salford Kidney Study were generated by Mann-Whitney U tests for continuous variables or χ2 test for categorical variables. Changes in the percentage of patients on RAASi (recorded as “yes” or “no”) were also assessed. All analyses were performed using IBM SPSS version 24 registered to the University of Manchester, Manchester, UK.
Results
From the 3,564 patients recruited into the Salford Kidney Study, 321 patients with CKD, T2DM, and hyperkalaemia receiving RAASi underwent propensity score matching with the 304 AMETHYST patients (online suppl. Fig. 1). Baseline demographics of patients with T2DM, CKD, and hyperkalaemia receiving RAASi are shown in Table 1 both before and after matching.
Prior to matching, the median age in the AMETHYST and the Salford Kidney Study subset was 68 (IQR 61–73) and 69 (IQR 61–75) years, respectively, with 63.2% and 63.6% of patients being male. Although all patients were receiving RAASi at baseline in both cohorts, patients in the AMETHYST cohort had significantly higher eGFR, systolic and diastolic BP, and frequency of HF at baseline but significantly lower sK+, compared with patients in the Salford Kidney Study.
Following propensity score matching to produce a cohort of 135:135 patients, no significant differences were observed in age, sex, systolic BP, prevalence of HF, sK+, or eGFR at baseline. However, significant differences remained for diastolic BP (84 [IQR 74–93] mm Hg in AMETHYST and 74 [IQR 61–80] mm Hg in the Salford Kidney Study).
At 12-month follow-up, sK+ was reduced from baseline in both cohorts (Fig. 1a). The reduction in sK+ was significantly greater in AMETHYST patients receiving patiromer compared with Salford Kidney Study patients, none of whom were receiving patiromer (−0.5 [IQR −0.9 to −0.1] mEq/L vs. −0.3 [IQR −0.5 to 0.1] mEq/L, respectively, p < 0.001).
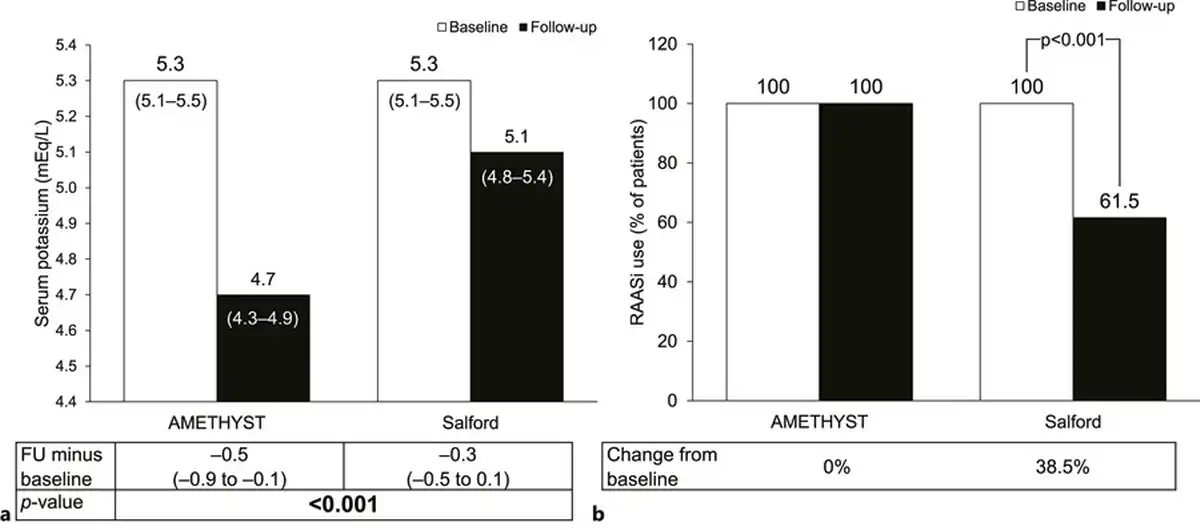
Fig. 1
Changes in serum potassium (a) and RAASi use (b) in AMETHYST and Salford Kidney Study cohorts at 12-month follow-up (matched sample). Serum potassium is expressed as median (IQR), and RAASi use is expressed as % of patients. p values were generated by Mann-Whitney U tests and χ2 test, respectively. FU, follow-up; IQR, interquartile range; RAASi, renin-angiotensin-aldosterone system inhibitor.
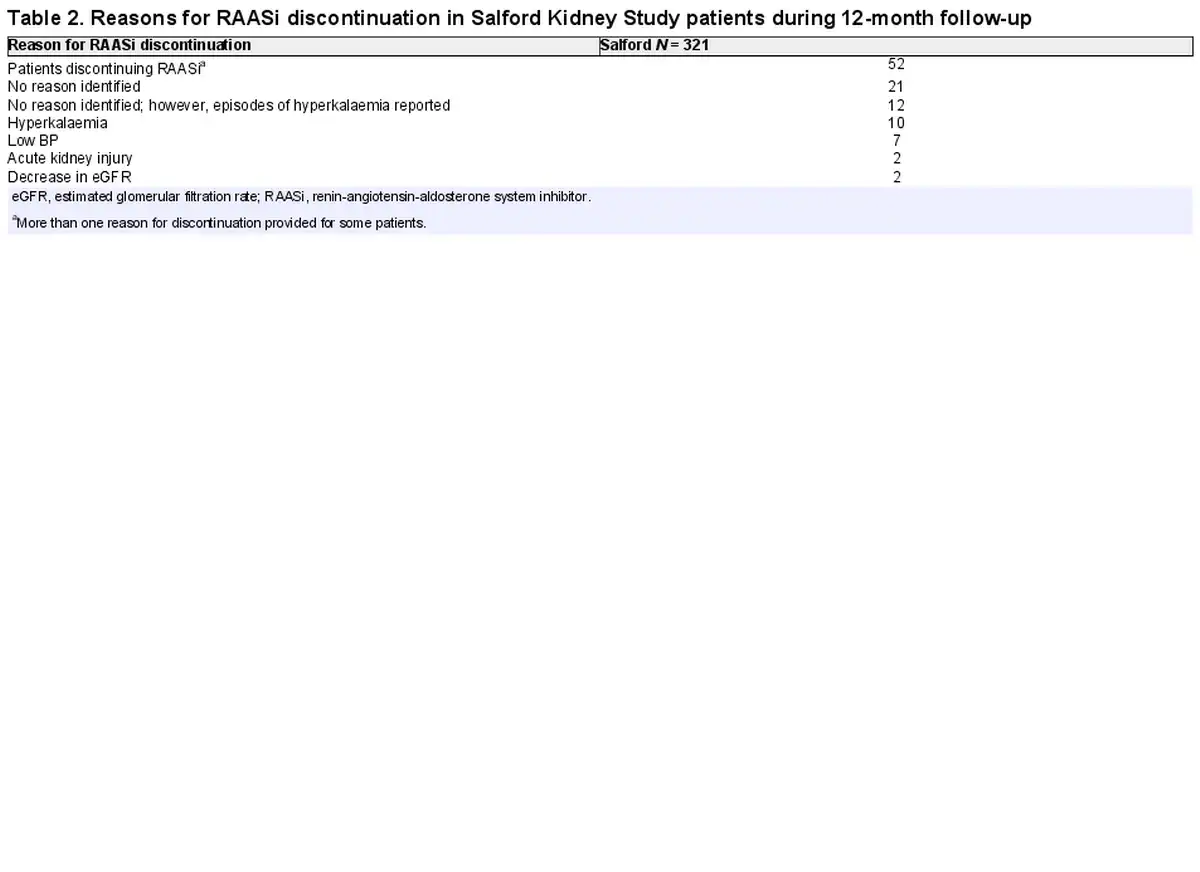
At follow-up, 100% of AMETHYST patients remained on RAASi treatment, whereas levels of RAASi use were reduced significantly by 38.5%, compared with baseline, in the Salford Kidney Cohort (p < 0.001) (Fig. 1b). The reasons for RAASi discontinuation are shown in Table 2. In total, 52 patients in the Salford Kidney Cohort had RAASi discontinued over the 12-month follow-up. Of these, hyperkalaemia was noted as a contributing factor for RAASi discontinuation in 22 patients (specifically, hyperkalaemia was stated directly as the reason for RAASi discontinuation in 10 patient records, while episode(s) of hyperkalaemia [sK+ >5.4 mEq/L] prior to discontinuation were noted in an additional 12 patient records). No reason or evidence of hyperkalaemia was identified in the records of 21 patients, while other less frequent reasons captured for RAASi discontinuation included low BP, low eGFR or decreases in eGFR, and acute kidney injury.
Reduction in systolic BP at follow-up was significantly greater in AMETHYST patients receiving patiromer compared with Salford Kidney Study patients not receiving patiromer (−15 [IQR −25 to −3] mm Hg vs. 1 [IQR −26 to 12] mm Hg, respectively, p = 0.002) (Fig. 2a). Similar results were observed for diastolic BP (−7 [IQR −16 to 3] mm Hg vs. −2 [IQR −11 to 7] mm Hg, respectively, p = 0.018) (Fig. 2b).
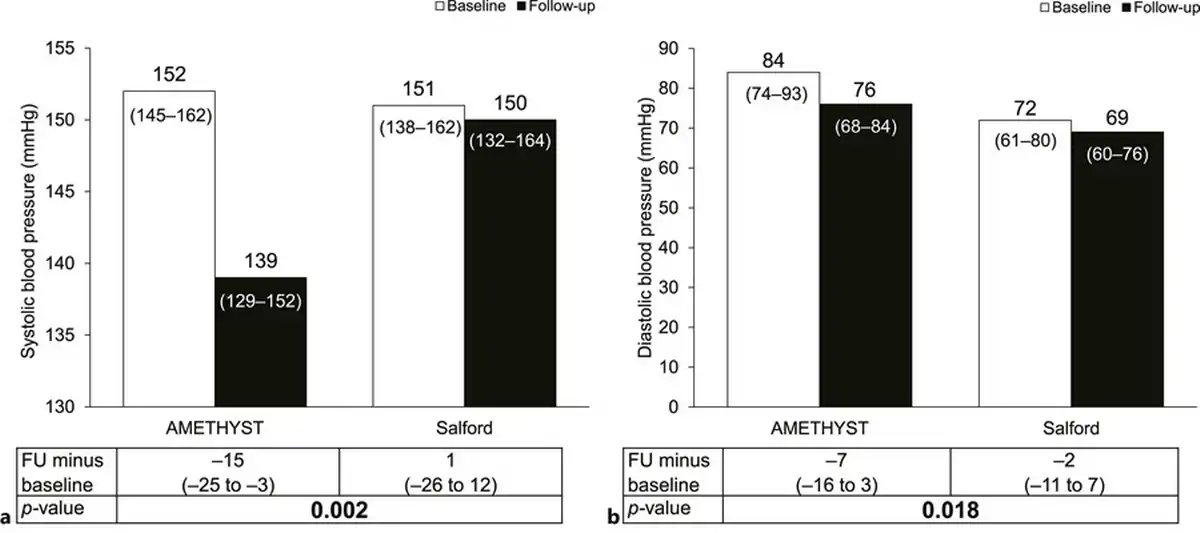
Fig. 2
Changes in systolic (a) and diastolic (b) BP in AMETHYST and Salford Kidney Study cohorts at 12-month follow-up (matched sample). Variables are expressed as median (IQR) and p values were generated by Mann-Whitney U tests. FU, follow-up; IQR, interquartile range.
Change in proteinuria, as measured by uACR, over the 12-month follow-up was not significantly different between AMETHYST and Salford Kidney Study patients (−7 [IQR −220 to 99] vs. 0.01 [IQR −106 to 170] mg/g, respectively, p = 0.093) (Fig. 3a). Similarly, no significant differences were observed for eGFR (−2 [IQR −7 to 10] vs. −2 [IQR −6 to 2] mL/min/1.73 m2, respectively, p = 0.169 (Fig. 3b).
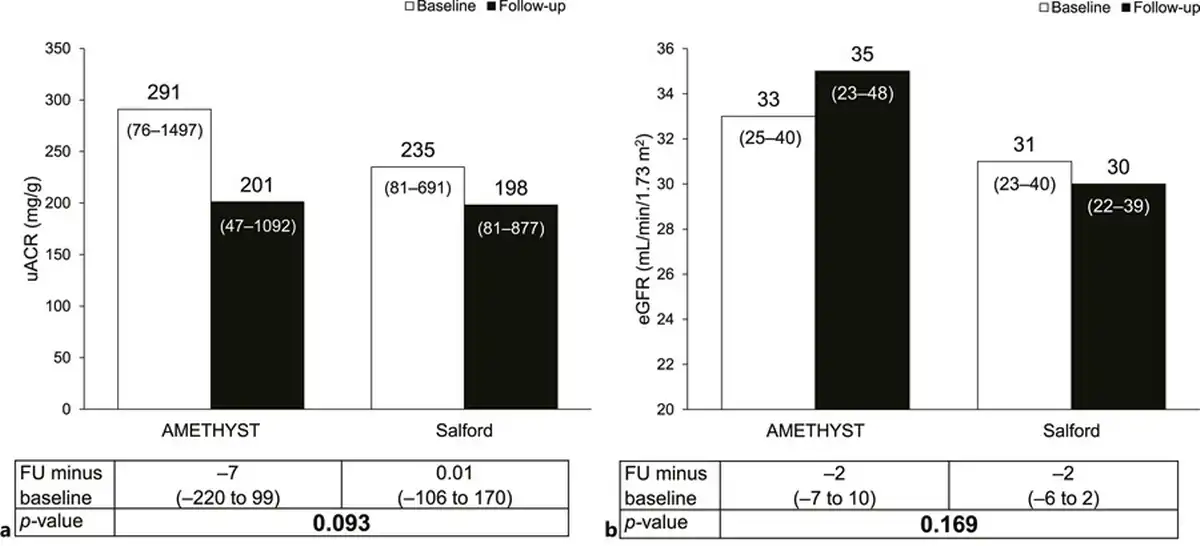
Fig. 3
Changes in uACR (a) and eGFR (b) in AMETHYST and Salford Kidney Study cohorts at 12-month follow-up (matched sample). Variables are expressed as median (IQR), and p values were generated by Mann-Whitney U tests. eGFR, estimated glomerular filtration rate; FU, follow-up; IQR, interquartile range; uACR, urine albumin-to-creatinine ratio.
Discussion
The overall aim of this study was to assess the impact of patiromer on the continuation of RAASi therapy in patients with CKD, T2DM, and hyperkalaemia enrolled in the AMETHYST trial, compared with a propensity score-matched, real-world cohort of patients not receiving patiromer from the Salford Kidney Study. Notably, this study found that in AMETHYST, sustained RAASi use was reported in 100% of patients receiving patiromer after 12 months, compared with 61.5% of patients in the Salford Kidney Study who did not receive patiromer. Of the 52 patients in the Salford Kidney Study who discontinued RAASi during the study period, discontinuation in 22 patients could be related to hyperkalaemia. A significantly greater reduction in sK+ was also observed in AMETHYST patients receiving patiromer compared with Salford Kidney Study patients. Simultaneous enablement of RAASi therapy and management of sK+ levels by patiromer, as shown in the current study, has previously been reported in other cardio-renal patient populations. For instance, the PEARL-HF trial found that in patients with chronic HF, and either a history of hyperkalaemia, leading to discontinuation of RAASi or beta-blocker therapy, or CKD treated with RAASi or beta-blocker therapy, patiromer significantly reduced the incidence of hyperkalaemia and enabled more patients to be treated with spironolactone, compared with placebo [, ]. Similarly, the OPAL-HK and AMBER trials reported RAASi enablement alongside a reduction in sK+ in patients with CKD and hyperkalaemia or resistant hypertension and advanced CKD, respectively [, , ]. Most recently, the DIAMOND trial demonstrated the ability of patiromer to enable RAASi optimization in 85% of patients with HF with reduced ejection fraction and either current or a history of RAASi-related hyperkalaemia, during a 12-week run-in period wherein all patients received patiromer []. The subsequent treatment phase of the DIAMOND trial, in which patients who achieved specified target doses of RAASi therapy during the run-in phase were randomized to either continue or withdraw from patiromer, additionally demonstrated the ability of patiromer to limit changes in sK+, number of HK events, and risk of mineralocorticoid receptor antagonist dose reduction []. The current study adds to this portfolio by demonstrating RAASi enablement alongside significant reductions in sK+ in patients with CKD, T2DM, and hyperkalaemia receiving patiromer as part of the AMETHYST trial, compared with propensity-matched patients not receiving patiromer in the real-world Salford Kidney Study. Although long-term outcomes were not studied in the current report, the clinical benefits of RAASi in both renal and cardiovascular diseases [–] and the detrimental effects of RAASi discontinuation [] are well established; therefore, these data suggest that enablement of RAASi treatment with patiromer has the potential to substantially benefit patient prognosis.
A secondary aim of the current analysis was to assess the impact of RAASi enablement with patiromer on BP and proteinuria. This study revealed a significantly greater reduction in systolic and diastolic BP in AMETHYST patients receiving patiromer, compared with Salford Kidney Study patients, although no significant differences in changes in eGFR or uACR were observed.
The mechanisms responsible for the beneficial effects of patiromer on both systolic and diastolic BP in the current study are likely secondary to the continuation of RAASi enabled by patiromer in the AMETHYST cohort. However, reductions in serum aldosterone with patiromer, as previously observed in the OPAL study [], could also be involved. Similarly, the limited improvements in BP observed in the Salford Kidney Study may reflect the haemodynamic effects of RAASi discontinuation, as previously reported following RAASi discontinuation in patients with CKD []. A statistically significant decrease in uACR was not observed between AMETHYST and Salford Kidney Study cohorts, potentially due to variation in the timing of RAASi discontinuation in patients in the Salford Kidney Cohort or the short length of follow-up. It is also possible that changes to eGFR may be hidden in Salford Kidney Study patients not receiving patiromer by the acute impact of discontinuing RAASi on eGFR [, ]; however, this is unclear. It is also worth noting that although RAASi dosage in AMETHYST was protocol mandated, modification of RAASi dosage in the Salford Kidney Study cohort was allowed as part of clinical care but would not have been captured by the binary RAASi (yes/no) analysis in the current study, potentially leading to increased variation within this dataset.
In 2020, a study by Ali and colleagues set a precedent for the use of propensity score matching analysis with the real-world Salford Kidney Study cohort to generate a placebo-like comparison arm for clinical trials studying hyperkalaemia []. In the study by Ali et al. [], propensity score matching with the Salford Kidney Study was used as substitute for a control arm to the OPAL-HK study to support the ability of patiromer to reduce sK+ in CKD patients on multiple RAASis. Compared with the current study, propensity score matching by Ali et al. was based on similar variables (except for diabetes status rather than baseline systolic BP and RAASi utilization) but included 87 precisely matched patients over a shorter follow-up of approximately 1 month [] to fit with the design of OPAL-HK.
Limitations of this study include the use of retrospective real-world data, which can be affected by a lack of quality in data recording. However, all data in this study were cross-checked to ensure all patients’ parameters were accurate at the point of entry into the analysis. It is also possible that a longer follow-up time and larger study numbers would have provided greater insight into changes of secondary outcome measures that may not have been captured with the current study design. Generalizability of data could be improved by the inclusion of patients from a wider range of ethnicities.
Overall, these data suggest that addition of patiromer to RAASi reduces sK+ levels and enables continuation of RAASi treatment in patients with CKD, T2DM, and hyperkalaemia over 1 year of follow-up. This study also revealed the beneficial impact of patiromer on systolic and diastolic BP, without substantial effects on eGFR or proteinuria, which may be secondary to RAASi enablement. Together, these results complement the growing portfolio of data demonstrating the benefits of patiromer for management of sK+ to enable RAASi use and further support the use of patiromer, alongside RAASi therapy, in patients with cardio-renal diseases.
Statement of Ethics
The Salford Kidney Study received ethical approval from the Northwest Greater Manchester South Research Ethics Committee (REC15/NW/0818). The AMETHYST study was conducted at 48 sites in 5 European countries. The protocol was approved by local or national independent ethics committees at each study site. Protocols were approved in line with International Conference on Harmonisation and Declaration of Helsinki principles, as well as local requirements. All patients in both studies provided written informed consent before any study-specific procedures were performed.
Conflict of Interest Statement
Rajkumar Chinnadurai and Sharmilee Rengarajan report no conflicts of interest. Jeffrey J. Budden and Carol Moreno Quinn report employment and shareholdings from CSL Vifor. Philip A. Kalra reports having received honoraria for lecturing and advisory board attendance from CSL Vifor and AstraZeneca and institutional research funding from CSL Vifor.
Funding Sources
This study was supported by Vifor Fresenius Medical Care Renal Pharma Ltd. Medical writing support was provided by Bethan Brown and Nicola Illingworth at AXON Communications (London) and funded by Vifor Fresenius Medical Care Renal Pharma Ltd.
Author Contributions
Rajkumar Chinnadurai, Sharmilee Rengarajan, Jeffrey J. Budden, Carol Moreno Quinn, and Philip A. Kalra: substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; and drafting the work or revising it critically for important intellectual content; and final approval of the version to be published; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
References
- 1. Maschio G, Alberti D, Janin G, Locatelli F, Mann JF, Motolese M, et al Effect of the angiotensin-converting-enzyme inhibitor benazepril on the progression of chronic renal insufficiency. The Angiotensin-Converting-Enzyme Inhibition in Progressive Renal Insufficiency Study Group N Engl J Med 1996 Apr 11 334 15 939–45
- 2. Ruggenenti P, Perna A, Gherardi G, Garini G, Zoccali C, Salvadori M, et al Renoprotective properties of ACE-inhibition in non-diabetic nephropathies with non-nephrotic proteinuria Lancet 1999 Jul 31 354 9176 359–64
- 3. Brenner BM, Cooper ME, de Zeeuw D, Keane WF, Mitch WE, Parving HH, et al Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy N Engl J Med 2001 Sep 20 345 12 861–9
- 4. Parving HH, Lehnert H, Bröchner-Mortensen J, Gomis R, Andersen S, Arner P The effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetes N Engl J Med 2001 Sep 20 345 12 870–8
- 5. Hou FF, Zhang X, Zhang GH, Xie D, Chen PY, Zhang WR, et al Efficacy and safety of benazepril for advanced chronic renal insufficiency N Engl J Med 2006 Jan 12 354 2 131–40
- 6. Lewis EJ, Hunsicker LG, Clarke WR, Berl T, Pohl MA, Lewis JB, et al Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes N Engl J Med 2001 Sep 20 345 12 851–60
- 8. Xie X, Liu Y, Perkovic V, Li X, Ninomiya T, Hou W, et al Renin–angiotensin system inhibitors and kidney and cardiovascular outcomes in patients with CKD: a Bayesian network meta-analysis of randomized clinical trials Am J Kidney Dis 2016 67 5 728–41
- 10. Kovesdy CP Management of hyperkalemia: an update for the internist Am J Med 2015 Dec 128 12 1281–7
- 11. Kim HW, Lee DH, Lee SA, Koh G A relationship between serum potassium concentration and insulin resistance in patients with type 2 diabetes mellitus Int Urol Nephrol 2015 Jun 47 6 991–9
- 12. Miao Y, Dobre D, Heerspink HJ, Brenner BM, Cooper ME, Parving HH, et al Increased serum potassium affects renal outcomes: a post hoc analysis of the Reduction of Endpoints in NIDDM with the Angiotensin II Antagonist Losartan (RENAAL) trial Diabetologia 2011 Jan 54 1 44–50
- 13. Collins AJ, Pitt B, Reaven N, Funk S, McGaughey K, Wilson D, et al Association of serum potassium with all-cause mortality in patients with and without heart failure, chronic kidney disease, and/or diabetes Am J Nephrol 2017 46 3 213–21
- 14. Hunter RW, Bailey MA Hyperkalemia: pathophysiology, risk factors and consequences Nephrol Dial Transplant 2019 Dec 1;34(Suppl 3):iii2–11
- 15. An JN, Lee JP, Jeon HJ, Kim DH, Oh YK, Kim YS, et al Severe hyperkalemia requiring hospitalization: predictors of mortality Crit Care 2012 Nov 21 16 6 R225
- 17. Kidney Disease Improving Global Outcomes (KDIGO) Diabetes Work Group KDIGO 2020 clinical practice guideline for diabetes management in chronic kidney disease Kidney Int 2020 Oct 98 4s S1–115
- 18. Li L, Harrison SD, Cope MJ, Park C, Lee L, Salaymeh F, et al Mechanism of action and pharmacology of patiromer, a nonabsorbed cross-linked polymer that lowers serum potassium concentration in patients with hyperkalemia J Cardiovasc Pharmacol Ther 2016 Sep 21 5 456–65
- 19. Pitt B, Anker SD, Bushinsky DA, Kitzman DW, Zannad F, Huang IZ, et al Evaluation of the efficacy and safety of RLY5016, a polymeric potassium binder, in a double-blind, placebo-controlled study in patients with chronic heart failure (the PEARL-HF) trial Eur Heart J 2011 Apr 32 7 820–8
- 20. Bakris GL, Pitt B, Weir MR, Freeman MW, Mayo MR, Garza D, et al Effect of patiromer on serum potassium level in patients with hyperkalemia and diabetic kidney disease: the AMETHYST-DN randomized clinical trial JAMA 2015 Jul 14 314 2 151–61
- 21. Pitt B, Bakris GL, Bushinsky DA, Garza D, Mayo MR, Stasiv Y, et al Effect of patiromer on reducing serum potassium and preventing recurrent hyperkalaemia in patients with heart failure and chronic kidney disease on RAAS inhibitors Eur J Heart Fail 2015 Oct 17 10 1057–65
- 22. Weir MR, Bakris GL, Bushinsky DA, Mayo MR, Garza D, Stasiv Y, et al Patiromer in patients with kidney disease and hyperkalemia receiving RAAS inhibitors N Engl J Med 2015 Jan 15 372 3 211–21
- 23. Pergola PE, Spiegel DM, Warren S, Yuan J, Weir MR Patiromer lowers serum potassium when taken without food: comparison to dosing with food from an open-label, randomized, parallel group hyperkalemia study Am J Nephrol 2017 46 4 323–32
- 24. Pitt B, Bushinsky DA, Kitzman DW, Ruschitzka F, Metra M, Filippatos G, et al Evaluation of an individualized dose titration regimen of patiromer to prevent hyperkalaemia in patients with heart failure and chronic kidney disease ESC Heart Fail 2018 Jun 5 3 257–66
- 25. Agarwal R, Rossignol P, Romero A, Garza D, Mayo MR, Warren S, et al Patiromer versus placebo to enable spironolactone use in patients with resistant hypertension and chronic kidney disease (AMBER): a phase 2, randomised, double-blind, placebo-controlled trial Lancet 2019 Oct 26 394 10208 1540–50
- 26. Butler J, Anker SD, Lund LH, Coats AJS, Filippatos G, Siddiqi TJ, et al Patiromer for the management of hyperkalemia in heart failure with reduced ejection fraction: the DIAMOND trial Eur Heart J 2022 Jul 28 43 41 4362–73
- 27. Weir MR, Bakris GL, Gross C, Mayo MR, Garza D, Stasiv Y, et al Treatment with patiromer decreases aldosterone in patients with chronic kidney disease and hyperkalemia on renin-angiotensin system inhibitors Kidney Int 2016 Sep 90 3 696–704
- 28. Hughes J, Chiu DYY, Kalra PA, Green D Prevalence and outcomes of proton pump inhibitor associated hypomagnesemia in chronic kidney disease PLoS One 2018 13 5 e0197400
- 29. Ahmed AK, Kamath NS, El Kossi M, El Nahas AM The impact of stopping inhibitors of the renin-angiotensin system in patients with advanced chronic kidney disease Nephrol Dial Transplant 2010 Dec 25 12 3977–82
- 30. Hansen HP, Rossing P, Tarnow L, Nielsen FS, Jensen BR, Parving HH Increased glomerular filtration rate after withdrawal of long-term antihypertensive treatment in diabetic nephropathy Kidney Int 1995 Jun 47 6 1726–31
- 31. Ali I, Chinnadurai R, Cornea G, Intorcia M, Kalra PA The role of patiromer: comparing OPAL-HK data with untreated real-world patients in the United Kingdom – A retrospective, propensity-matched analysis PLoS One 2020 15 8 e0237467
- 7. Heart Outcomes Prevention Evaluation Study Investigators Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus: results of the HOPE study and MICRO-HOPE substudy Lancet 2000 Jan 22 355 9200 253–9.
- 9. Dunn JD, Benton WW, Orozco-Torrentera E, Adamson RT The burden of hyperkalemia in patients with cardiovascular and renal disease Am J Manag Care 2015 Nov 21 15 Suppl l s307–15.
- 16. Epstein M, Reaven NL, Funk SE, McGaughey KJ, Oestreicher N, Knispel J Evaluation of the treatment gap between clinical guidelines and the utilization of renin-angiotensin-aldosterone system inhibitors Am J Manag Care 2015 Sep 21 11 Suppl l S212–20.