Introduction
Erosive tooth wear (ETW) is a process of loss of the tooth structure whose primary etiological factor is tooth erosion (chemical loss due to acids), which may be associated with attrition and/or abrasion [Schlueter et al., 2020]. Recent studies have shown high prevalence rates of ETW in children (62%) [Garduno-Picazo et al., 2020], adolescents (57%) [Racki et al., 2020], and adults (97.9%) [Marró et al., 2020], which justifies the identification of the associated factors to prevent its occurrence/progression. The clinical diagnosis of ETW is relevant during adolescence when potential risk factors may be under development, such as higher consumption of soft drinks, eating disorders, and behavioral changes related to oral care. In addition, considering the lifetime of permanent teeth and the progressive nature of ETW, its diagnosis in young populations and in the early stages of wear is of special interest.
One of the factors that may be related to the occurrence of ETW is oral hygiene practices, due to the synergistic effect between the processes of erosion and abrasion as the enamel softened by the erosive challenge is influenced by mechanical factors, such as abrasion, resulting in greater loss of dental hard tissues [Eisenburger et al., 2003]. In addition to variables related to the individual, such as brushing method, force, time, and frequency, factors related to the toothpaste (abrasiveness) and toothbrush (type of brush, filament end-rounding, and filament stiffness) have also been investigated. In this sense, toothbrush bristle stiffness has been suggested as a potential factor associated with ETW prevalence [Addy and Hunter, 2003; Wiegand et al., 2008; Lippert et al., 2017].
Just 3 cross-sectional studies assessed the association between bristle stiffness and ETW [Nahás Pires Corrêa et al., 2011; Haneet and Vandana, 2015; Wei et al., 2016]. One study including 404 Indian individuals aged 16–55 years found an association between toothbrushes with medium-hardness bristles and erosion-abrasion [Haneet and Vandana, 2015]. In the same way [Wei et al., 2016], assessing 720 participants aged 36–74 years from China demonstrated a higher probability of dentin exposure due to tooth wear among those who used a toothbrush with hard bristles [Wei et al., 2016]. On the other hand, no association was found between bristle stiffness and ETW in a convenience sample of Brazilian children and adolescents [Nahás Pires Corrêa et al., 2011]. To the best of our knowledge, there is no study addressing this issue in a population-based representative sample of adolescents.
Considering the scarce evidence on this topic, the aim of this study was to investigate the association between toothbrush bristle stiffness and the occurrence of ETW among 15- to 19-year-old adolescents from southern Brazil. We hypothesized that adolescents who used toothbrushes with harder bristles would be more affected by ETW than those who used softer toothbrushes.
Subjects and Methods
Study Design and Sample
A population-based cross-sectional study was carried out to assess the oral health status of adolescents aged 15–19 years from Santa Maria, a mid-sized city located in southern Brazil. A previous article on the association between sociodemographic variables and ETW in this population has been published elsewhere [Racki et al., 2020] and provides more detailed information on the sampling strategy and the examiners’ reproducibility.
In brief, a sample of 1,066 students was estimated for the present study (50% prevalence, 95% confidence interval [CI], 80% power, and 3% precision). A nonparticipation rate of 50% was factored in, totaling 1,600 adolescents to be invited to participate. Adolescents born in the years 1999–2003 who were attending any school period (morning, afternoon, or night) were considered eligible. Individuals using fixed orthodontic appliances or those presenting special needs were not included. All the 37 high schools in the municipality were invited to participate in the study (26 public and 11 private).
Data Collection
Data collection was conducted from March to November 2018 and included 2 questionnaires and clinical examination. One questionnaire was sent to the parents/legal guardians of the selected students, containing questions on sociodemographic information (sex, age, and socioeconomic status [SES]). The second questionnaire was applied to the students to collect data regarding oral hygiene habits (toothbrushing frequency, toothbrushing after meals, and toothbrush bristle stiffness) and dietary habits focusing on the frequency of consumption of acid beverages (soft drinks, citric fruits, and fruit juice).
Clinical examination was performed in a room provided by the school, with the students in a supine position. Students cleaned their teeth with toothbrush, toothpaste, and dental floss provided by the research team. The examiner used to check the quality of tooth cleaning and complemented it, when needed. After isolation with cotton rolls and drying with a portable compressor, all erupted permanent teeth were assessed and classified according to the Basic Erosive Wear Examination (BEWE) [Bartlett et al., 2008], except third molars. BEWE classifies free surfaces into 4 scores, as follows: 0, without erosive wear; 1, initial loss of surface texture; 2, distinct defect, hard tissue loss <50% of the surface area; and 3, distinct defect, hard tissue loss ≥50% of the surface area. The diagnostic criteria were based on clinical characteristics such as smoothness and surface shine, presence of perikymata, lesion localization, presence of flattened convex areas or concavities where the width clearly exceeds the depth, and features of the cups and incisal edges [Lussi et al., 2006]. Two trained and calibrated examiners (minimal kappa value of 0.75) performed the clinical examinations, as previously described [Racki et al., 2020].
Data Analysis
The outcome of this study was ETW prevalence, defined as the percentage of individuals with at least 1 tooth with BEWE ≥1. The main predictor variable was toothbrush bristle stiffness, classified as extra-soft, soft, medium, or hard.
Adjusting variables included potential risk factors to ETW such as sociodemographic data, toothbrushing frequency, toothbrushing after meals, and dietary habits. Sociodemographic variables were sex (boys vs. girls), age (≤16 vs. ≥17 years), and SES. Using cutoff points proposed by the standard Brazilian economic classification [ABEP, 2015], households were classified into low (≤16 points, corresponding to social classes D and E), mid-low (≥17 to ≤22 points, corresponding to social class C2), mid-high (≥23 to ≤28 points, corresponding to social class C1), or high (≥29 points, corresponding to social classes A, B1, and B2) SES. Toothbrushing frequency was classified as ≤ once/day versus twice/day or ≥3 times/day, while toothbrushing after meals was dichotomized as “no” or “yes.” Dietary habits were classified as nondaily versus daily.
Data analysis was performed using Stata software (Stata 14.2 for Windows; Stata Corporation, College Station, TX, USA) and using survey commands that took into account the survey design, including clustering, stratification, weighting, and robust variance estimation. A weight variable based on the probability of selection and population distribution according to sex and school type was used to adjust for the potential bias in the population estimates [Korn and Graubard, 1999]. Preliminary analysis comparing the ETW prevalence by predictor variables was performed using the Wald test.
The association between predictor variables and ETW prevalence was assessed using Poisson regression models. The prevalence ratios (PRs) and their respective 95% CI were estimated. Predictor variables presenting a p value <0.15 in the unadjusted analysis were selected for inclusion in the adjusted model. The level of significance was set at 5%.
Results
A total of 1,197 out of 1,656 adolescents were examined, yielding a participation rate of 72.3%. A prevalence of 57% (95% CI = 52.5–61.5) was observed, corresponding to 675 adolescents.
Table 1 presents the sample distribution, ETW prevalence, and its association with predictor variables. Adolescents who reported the use of toothbrushes with soft or medium bristles had a higher ETW prevalence than their counterparts reporting the use of extra-soft toothbrushes (p < 0.05). No difference was found regarding toothbrushes with hard bristles (p > 0.05). ETW prevalence also differed significantly between categories of sex, SES, and toothbrushing frequency.
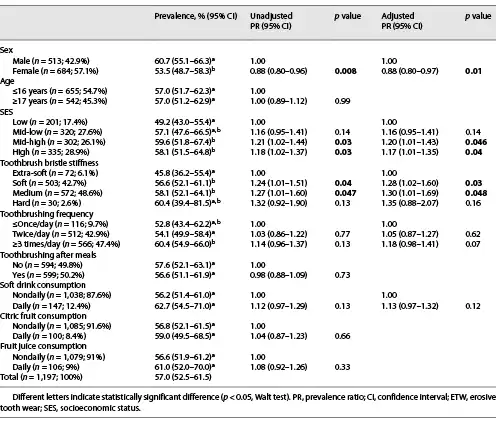
The toothbrush bristle stiffness was associated with ETW prevalence in both unadjusted and adjusted analyses. The final model showed that individuals who used toothbrushes with soft (PR = 1.28, 95% CI = 1.02–1.60) or medium (PR = 1.30, 95% CI = 1.01–1.69) bristles were around 30% more likely to have ETW than those who used toothbrushes with extra-soft bristles. The category hard bristles has not reached statistical significance. In addition, sex (boys) and SES (mid-high and high) were significantly associated with the study outcome.
Discussion
The present study investigated the association between toothbrush bristle stiffness and ETW in a representative sample of 15- to 19-year-old adolescents from southern Brazil. The results showed that the toothbrushes with soft or medium bristles were significantly associated with ETW prevalence, affording an increased risk for ETW compared with the extra-soft toothbrush. To the best of our knowledge, this is the first study addressing this topic at the population level among adolescents.
Few studies have assessed the relationship between toothbrush bristle stiffness and ETW, most of them being conducted using in vitro methodologies. Two experiments found no significant difference in tissue loss between toothbrushes with soft and hard bristles [Voronets et al., 2008] nor among soft, medium, and hard bristles [Bizhang et al., 2016]. A recent in vitro study evaluating the effect of different types of manual toothbrushes (ultrasoft, soft, medium, or hard) and different brushing loads (1.5 N and 3 N) found no association between the type of toothbrush and surface loss on enamel; however, brushing with a hard bristle toothbrush at brushing loads of 1.5 N resulted in higher enamel loss [Souza et al., 2021]. Two other studies demonstrated that the softened enamel is significantly influenced by the abrasiveness of the toothpaste and that the brush filament stiffness acts as a modulator of this process [Wiegand et al., 2008; Lippert et al., 2017] with this interaction being more relevant for dentin than for enamel [Lippert et al., 2017]. The present study demonstrated that the use of toothbrushes with extra-soft bristles was associated with a lower prevalence of ETW than soft or medium bristles. The disagreement between these in vitro studies and the present investigation may be related to the different study designs. The interaction of important factors in the oral environment and the sustainability of the enamel may influence the individual susceptibility to ETW [Uhlen et al., 2016] and may be not fully reproduced using in vitro methodologies.
Two other cross-sectional studies have also found an association between toothbrush bristle stiffness and ETW [Haneet and Vandana, 2015; Wei et al., 2016]. Wei et al. [2016] demonstrated that toothbrushes with hard bristles were associated with a higher probability of dentin exposure due to ETW than soft bristles among Chinese adults aged 36–74 years (p = 0.003). This study showed that the type of bristles was also responsible for a greater severity of ETW (dentin exposure). The other study by Haneet and Vandana [2015] showed that the medium-hardness bristles were significantly associated with abrasion/erosion in a population of 16- to 55-year-old Indians. The lack of association with toothbrushes with hard bristles found in their study may be attributed to the reduced number of individuals in this category (n = 21), which may have reduced the statistical power of the analysis. The same obstacle appears to have occurred in the present sample of Brazilian adolescents, since only 30 individuals reported the use of toothbrushes with hard bristles, and this category has not reached statistical significance. Controversially, the other cross-sectional study available in the literature did not find an association between toothbrush bristle stiffness and ETW [Nahás Pires Corrêa et al., 2011], which may be related to the reduced sample size (n = 232), with only 94 individuals with permanent dentition.
In relation to the adjusting variables, we found significant associations with sex (boys) and SES (mid-high and high), corroborating the previous literature on this topic. Boys have been consistently found to be more likely to have ETW than girls [Dugmore and Rock, 2004; Alvarez Loureiro et al., 2015; Alves et al., 2015; Brusius et al., 2018], which may be related to dietary preferences, bite force, greater consumption of sports drinks, and greater practice of physical activities. The socioeconomic conditions in which individuals find themselves may be responsible for a greater susceptibility of some individuals to develop diseases than others. It can be assumed that the mechanisms by which socioeconomic factors influence the occurrence of ETW are related to dietary patterns and lifestyle [Racki et al., 2020]. The lack of association between toothbrushing frequency and ETW is in agreement with the literature [Al-Dlaigan et al., 2002; Alvarez Loureiro et al., 2015; Alves et al., 2015; Brusius et al., 2018] as well as the relationship between brushing after meals and ETW [Hong et al., 2020]. Unlike shown by Chan et al. [2020] in a recent systematic review, no association was found between consumption of soft drinks and ETW in this adolescent population.
It is well known that BEWE is a scoring system that records the most severely affected surface in a sextant and uses the cumulative score to define risk levels and guide the clinical management of ETW [Bartlett et al., 2008]. In the present study however, we chose to define a binary outcome based on ETW prevalence (% of adolescents with at least 1 tooth with BEWE ≥1), instead of using the previously defined BEWE categories. Considering the age-group under investigation, we believe that the detection of any sign of ETW may be clinically relevant throughout life and that individuals with cumulative scores of 1 or 2 should not be combined with individuals free of ETW in the same category (risk level: “none”), as originally recommended.
The strengths of this study include the representative sample of the population, with a defined and uniform age-group (adolescents of 15–19 years old), thus facilitating the data analysis and the interpretation of the study findings. Contradictorily, the other cross-sectional studies by Haneet and Vandana [2015] and Wei et al. [2016] included a wide age-group, making it difficult to distinguish pathological ETW from physiological aging of the tooth structures. In addition, our study was the first population-based cross-sectional study to include extra-soft toothbrushes and to find a difference between this and the other types of bristle stiffness. Data on the type of toothbrush individuals used were collected by a self-completed questionnaire, which could be seen as a possible limitation of our study as well as the lack of data on other oral hygiene-related variables that could influence or modulate ETW occurrence, mainly the toothpaste abrasiveness and the brushing technique and force.
In conclusion, this population-based cross-sectional study found a very weak but significant association between toothbrush bristle stiffness and ETW among Brazilian adolescents. Considering the cross-sectional design of this study and considering that some association was found even in such a young population, future studies using different designs and including different age-groups might elucidate the clinical relevance of this finding.
Acknowledgments
We would like to thank all volunteers, their parents/legal guardians, and the schools for their contribution.
Statement of Ethics
The study protocol was approved by the Ethics Committee of the Federal University of Santa Maria, Brazil (Protocol Number 2.178.299). The research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki. All patients or their legal guardians signed a written informed consent form. Students received a report of their oral health status and were referred to dental treatment when necessary.
Conflict of Interest Statement
The authors have no conflicts of interest to declare.
Funding Sources
This study was supported by the Federal University of Santa Maria, the Municipality Oral Health Policy of Santa Maria, and the National Coordination of Post-Graduate Education, Ministry of Education, Brazil (funding code 001).
Author Contributions
Débora N.O. Racki contributed to data collection, data analysis, and paper writing. Letícia D. Comim and Ângela Dalla Nora contributed to data collection and data analysis. Júlio Eduardo A. Zenkner and Luana S. Alves contributed to study design, data analysis, and paper writing.
Data Availability Statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
References
- 1. Associação Brasileira de Empresas de Pesquisa. Standard Brazilian economic classification. Brazil: ABEP; 2015.
- 2. Addy M, Hunter ML. Can tooth brushing damage your health? Effects on oral and dental tissues. Int Dent J. 2003;53(Suppl 3):177–86. http://dx.doi.org/10.1111/j.1875-595x.2003.tb00768.x.
- 3. Al-Dlaigan YH, Shaw L, Smith AJ. Dental erosion in a group of British 14-year-old, schoolchildren. Part III: influence of oral hygiene practices. Br Dent J. 2002;192(9):526–30.
- 4. Alvarez Loureiro L, Fabruccini Fager A, Alves LS, Alvarez Vaz R, Maltz M. Erosive tooth wear among 12-year-old schoolchildren: a population-based cross-sectional study in Montevideo, Uruguay. Caries Res. 2015;49(3):216–25.
- 5. Alves LS, Brusius CD, Damé-Teixeira N, Maltz M, Susin C. Dental erosion among 12-year-old schoolchildren: a population-based cross-sectional study in South Brazil. Int Dent J. 2015;65(6):322–30. http://dx.doi.org/10.1111/idj.12189.
- 6. Bartlett D, Ganss C, Lussi A. Basic erosive wear examination (BEWE): a new scoring system for scientific and clinical needs. Clin Oral Investig. 2008;12(1):S65–8. http://dx.doi.org/10.1007/s00784-007-0181-5.
- 7. Bizhang M, Riemer K, Arnold WH, Domin J, Zimmer S. Influence of bristle stiffness of manual toothbrushes on eroded and sound human dentin – an in vitro study. PLoS One. 2016;11(4):e0153250–13. http://dx.doi.org/10.1371/journal.pone.0153250.
- 8. Brusius CD, Alves LS, Susin C, Maltz M. Dental erosion among South Brazilian adolescents: a 2.5-year longitudinal study. Community Dent Oral Epidemiol. 2018;46(1):17–23. http://dx.doi.org/10.1111/cdoe.12322.
- 9. Chan AS, Tran TTK, Hsu YH, Liu SYS, Kroon J. A systematic review of dietary acids and habits on dental erosion in adolescents. Int J Paediatr Dent. 2020;30(6):713–33. http://dx.doi.org/10.1111/ipd.12643.
- 10. Dugmore CR, Rock WP. The prevalence of tooth erosion in 12-year-old children. Br Dent J. 2004;196(5):279–3. http://dx.doi.org/10.1038/sj.bdj.4811040.
- 11. Eisenburger M, Shellis RP, Addy M. Comparative study of wear of enamel induced by alternating and simultaneous combinations of abrasion and erosion in vitro. Caries Res. 2003;37(6):450–5. http://dx.doi.org/10.1159/000073399.2003
- 12. Garduno-Picazo MV, Ruiz-Ramos M, Juárez-López MLA. Dental erosion risk factors in 6–12 year old children in Mexico city. J Clin Pediatr Dent. 2020;44(2):95–9.
- 13. Haneet RK, Vandana LK. Prevalence of dentinal hypersensitivity and study of associated factors: a cross-sectional study based on the general dental population of Davangere, Karnataka, India. Int Dent J. 2015;66(1):49–57.
- 14. Hong DW, Lin XJ, Wiegand A, Yu H. Does delayed toothbrushing after the consumption of erosive foodstuffs or beverages decrease erosive tooth wear? A systematic review and meta-analysis. Clin Oral Investig. 2020;24(12):4169–83. http://dx.doi.org/10.1007/s00784-020-03614-9.
- 15. Korn B, Graubard E. Analysis of health surveys. New York; 1999.
- 16. Lippert F, Arrageg MA, Eckert GJ, Hara AT. Interaction between toothpaste abrasivity and toothbrush filament stiffness on the development of erosive/abrasive lesions in vitro. Int Dent J. 2017;67(6):344–50. http://dx.doi.org/10.1111/idj.12305.
- 17. Lussi A, Hellwig E, Zero D, Jaeggi T. Erosive tooth wear: diagnosis, risk factors and prevention. Am J Dent. 2006;19(6):319–25.
- 18. Marró ML, Aránguiz V, Ramirez V, Lussi A. Prevalence of erosive tooth wear in Chilean adults, 2016: a cross-sectional study. J Oral Rehabil. 2020;47(4):467–72. http://dx.doi.org/10.1111/joor.12922.
- 19. Nahás Pires Corrêa MS, Nahás Pires Corrêa F, Nahás Pires Corrêa JPJP, Murakami C, Mendes FM. Prevalence and associated factors of dental erosion in children and adolescents of a private dental practice. Int J Paediatr Dent. 2011;21(6):451–8. http://dx.doi.org/10.1111/j.1365-263X.2011.01150.x.
- 20. Racki DNO, Dalla Nora Â, Comim LD, Zenkner JEDA, Alves LS. Erosive tooth wear among South Brazilian adolescents, and its association with sociodemographic variables. Braz Oral Res. 2020;33(119):e119–11. http://dx.doi.org/10.1590/1807-3107bor-2019.vol33.0119.
- 21. Schlueter N, Amaechi BT, Bartlett D, Buzalaf MAR, Carvalho TS, Ganss C, et al. Terminology of erosive tooth wear: consensus report of a workshop organized by the ORCA and the cariology research group of the IADR. Caries Res. 2020;54(1):2–6. http://dx.doi.org/10.1159/000503308.
- 22. Souza CMS, Sakae LO, Carneiro PMA, Esteves RA, Scaramucci T. Interplay between different manual toothbrushes and brushing loads on erosive tooth wear. J Dent. 2021;105(1):103577–81. http://dx.doi.org/10.1016/j.jdent.2020.103577.
- 23. Uhlen MM, Mulic A, Holme B, Tveit AB, Stenhagen KR. The susceptibility to dental erosion differs among individuals. Caries Res. 2016;50(2):117–23. http://dx.doi.org/10.1159/000444400.
- 24. Voronets J, Jaeggi T, Buergin W, Lussi A. Controlled toothbrush abrasion of softened human enamel. Caries Res. 2008;42(4):286–90. http://dx.doi.org/10.1159/000148160.
- 25. Wei Z, Du Y, Zhang J, Tai B, Du M, Jiang H. Prevalence and indicators of tooth wear among Chinese adults. PLoS One. 2016;11(9):1–14.
- 26. Wiegand A, Schwerzmann M, Sener B, Magalhaes AC, Roos M, Ziebolz D, et al. Impact of toothpaste slurry abrasivity and toothbrush filament stiffness on abrasion of eroded enamel – an in vitro study. Acta Odontol Scand. 2008;66(4):231–5. http://dx.doi.org/10.1080/00016350802195041.