What was known before
Decreased physical activity and increased sedentary behavior are associated with poor health outcomes in the general population. Hemodialysis patients have considerably reduced physical activity compared with nondialysis populations but less is known about their sedentary tendencies and locations where these behaviors occur.
What this adds
This study shows that hemodialysis patients exhibit minimal physical activity, and substantial sedentary behavior, across a limited range of locations. Given the sedentary tendencies of this population, future studies should focus on increasing physical activity at any location frequented. Home-based exercise programs may serve as a potential adjunct to intradialytic-based therapies given the considerable amount of time spent in the home environment.
Introduction
Patients receiving dialysis have reduced levels of physical activity and increased sedentary behavior compared with the general population., This is associated with a negative impact on survival for those receiving dialysis,- whereas habitual physical activity may confer a survival advantage,,- and improved health-related quality of life among in-center hemodialysis patients.
Questionnaire-based assessments have shown low self-reported physical activity in hemodialysis patients., Although important, these evaluations require introspective ability and may suffer from response bias which may limit objectivity of the data collected. They also may not accurately capture details such as intensity, timing, and duration of physical activity. As such, there has been a greater emphasis on the use of objective accelerometer-based assessments of physical activity in dialysis populations.,,, Accelerometers can further stratify physical activity into moderate to vigorous physical activity, and light physical activity, based on number of counts per minute. Accelerometer-based studies confirm that dialysis patients are less active compared with healthy controls and renal transplant recipients. Much less is known about the prevalence of sedentary behavior in hemodialysis patients using objective accelerometer-based assessment. This is especially relevant when considering the association between sedentary behavior and poor outcomes, including cardiovascular disease and all-cause mortality, in other nondialysis patient populations. The role of hemodialysis treatment also needs to be considered when assessing sedentary behavior, as prior studies have shown lower physical activity on dialysis days compared with nondialysis days.
Identifying locations where physical activity and sedentary behavior occur is an essential step in developing interventions targeting these behaviors in the hemodialysis population. Previous studies have shown that the majority of moderate to vigorous physical activity in the general population occurs outside of the home environment., However, this population does not have the same degree of comorbidity and frailty as individuals who require in-center hemodialysis which limits the generalizability of these findings. Up to 67% of dialysis patients met the definition of frailty including poor self-reported physical functioning, fatigue/exhaustion, and undernutrition in a recent study which suggests their physical activity tendencies may not mirror those of the general population. Determining where physical activity and sedentary behavior occur for hemodialysis patients is the first step to designing successful interventions which modify these behaviors. To date, objective assessments of real-world locations where physical activity and sedentary behavior occur have not been examined in a hemodialysis population.
Therefore, in a cohort of in-center hemodialysis patients, the purpose of this study was to (1) objectively determine the minutes per day of moderate to vigorous physical activity, light physical activity, and sedentary behavior; (2) describe differences in moderate to vigorous physical activity, light physical activity, and sedentary behavior comparing dialysis versus nondialysis days; and (3) describe the locations where moderate to vigorous physical activity, light physical activity, and sedentary behavior occur using global positioning system (GPS) data. We hypothesized that hemodialysis patients would exhibit a low level of moderate to vigorous physical activity and high sedentary behavior given the results of prior questionnaire-based activity assessments and that sedentary behavior would be higher on dialysis days. We also hypothesized that physical activity would occur most frequently in the home environment given the frailty of this population.
Methods
Population
We analyzed a cross section of chronic in-center hemodialysis patients at a large tertiary care institute (Queen Elizabeth II Health Science Centre, Halifax, NS). Recruitment occurred over a 3-month period between June 1, 2017, and August 31, 2017. We chose a convenience sample of any patient who consented to participate and satisfied inclusion and exclusion criteria. The Nova Scotia Health Authority Research Ethics Board (#1022204) approved this study. All participants provided written informed consent.
Inclusion/Exclusion
Eligible patients were ≥18 years old, receiving in-center hemodialysis for at least 3 months, and could read and write in English, to ensure accurate usage of the accelerometer and GPS unit. We excluded any patient who was admitted to hospital, receiving acute dialysis with anticipation of renal recovery, those who were unable to participate due to medical or physical limitation (bed ridden, amputation without prosthesis, wheelchair bound, or unable to ambulate despite gait aids), or those that were deemed by their primary nephrologist to be unlikely to collect the requisite number of days of accelerometer data required for the study.
Procedure
Patients were provided instruction on accelerometer and GPS use by study coordinators and asked to wear both devices continuously (from waking until bed) for a duration of 9 days. We chose this duration to account for incomplete data capture on the days that the devices were collected and returned with a goal of 7 complete days of accelerometer/GPS wear time. Furthermore, this timeline allowed for 3 dialysis sessions to be captured representing a typical week for hemodialysis patients. The accelerometer (3.8 × 3.7 × 1.8 cm) was attached to a belt and worn at the hip while the GPS unit (7.2 × 4.6 × 2 cm) was stored in a belt pouch on the contralateral hip. Devices were not worn overnight or during water-based activities.
Accelerometer-Measured Physical Activity and Sedentary Behavior
Physical activity and sedentary behavior were measured using the Actigraph GT3X accelerometer, which has been shown to be a valid and reliable tool., Data were collected in 5-second epochs and reintegrated to a 60-second epoch prior to being cleaned using Actilife 6.10.2 software (Actigraph, LLC). Nonwear time was defined as at least 90 consecutive minutes of zero counts, with allowance for up to 2 minutes of nonzero counts provided there are no counts recorded in the 30 minutes upstream and downstream from the nonzero interval. A valid day was subsequently defined as ≥10 hours of wear time. Definitions of moderate to vigorous physical activity, light physical activity, and sedentary behavior were activities that require ≥3 metabolic equivalents (METs), 1.6 to 2.9 METs, and ≤1.5 METs in a sitting, reclining, or lying posture, respectively. Examples include raking the lawn (moderate to vigorous physical activity), watering plants (light physical activity), and watching TV on the couch (sedentary behavior). The Troiano et al cut-points were used to define sedentary behavior (<100 counts per minute), light physical activity (100-2019 counts per minute), and moderate to vigorous physical activity (≥2020 counts per minute).
Geographical Locations of Physical Activity and Sedentary Behavior
Locations where physical activity and sedentary behavior occurred were mapped objectively using the Qstarz BT-Q1000X GPS data logger, which provided the date, time, speed, latitude, and longitude information every 5 seconds (ie, to be in sync with the accelerometer data). This device is accurate within a 3-meter distance of the participant and has been shown to be a valid tool., The device was capable of recording up to 24 hours of location data per day but needed to be recharged by patients on a nightly basis. Using the Actilife 6.10.2 software, the 60-second epoch accelerometer data were linked to the 5 second GPS data and imported into ArcGIS 10.2.2. The linked data were then geocoded using OpenStreetMaps and World Imagery base maps in addition to the Google Maps add-in, which provided a street view when needed. Each minute of linked data was coded into home, a residence that was not home (eg, a neighbor’s house), a hospital or medical clinic, a street or sidewalk, a walking path or trail, a food or shopping area (eg, a restaurant, a mall), greenspace and/or recreation area (eg, a park, fitness facility, field, etc), a service building (eg, a bank, car dealership, a movie theater, etc), and transportation (eg, driving 80 miles/hour on the highway while sedentary), and error (eg, GPS points in the ocean).
Patient Characteristics
Baseline demographics were obtained following a questionnaire and assessment of patient electronic records and paper charts at the time of consent.
Analysis
Baseline demographics and characteristics for the entire study cohort were reported using descriptive statistics. Mean with standard deviation, median with interquartile range, and number with percent were used for continuous normal, nonnormal, and categorical baseline variables, respectively. Time spent in sedentary behavior, light physical activity, and moderate to vigorous physical activity was averaged across valid days to give total minutes per day at each activity level and reported as medians with interquartile ranges. The proportion of time spent in each state was reported as a percentage of total wear time. In the primary analysis and consistent with recommendations, at least 4 valid days were required for reporting of accelerometer data and for GPS linkage. The amount of moderate to vigorous physical activity accumulated in bouts of ≥10 minutes was used to determine whether individuals were meeting the Canadian physical activity guidelines (weekly sum ≥ 150 minutes of moderate to vigorous physical activity in bouts of ≥ 10 minutes). To count as a bout, 10 consecutive minutes of observations had to exceed the moderate to vigorous physical activity cut-point, with allowance for a maximum of 2 observations falling below the cut-point during that period (ie, 8 out of 10 minutes had to be above the cut-point). If patients had 1 to 6 valid days, their average daily moderate to vigorous physical activity was multiplied by 7 to obtain a weekly sum. For the analysis evaluating differences in time spent in sedentary behavior, light physical activity, and moderate to vigorous physical activity comparing dialysis with nondialysis days, we reported time and percentage of daily wear time in each activity state. Unadjusted comparisons were made using the Wilcoxon rank sum test. The percent of total linked time at a given location was reported for overall accelerometer use and each activity level. Similar to above, the percent of daily linked time at a given location was compared for dialysis versus nondialysis days using the rank sum test. For all analyses, a P < .05 was used as the threshold for statistical significance. All statistical analyses were conducted using Stata 14 software (Stata Statistical Software: Release 14, College Station TX: StataCorp LP).
Results
Baseline Characteristics
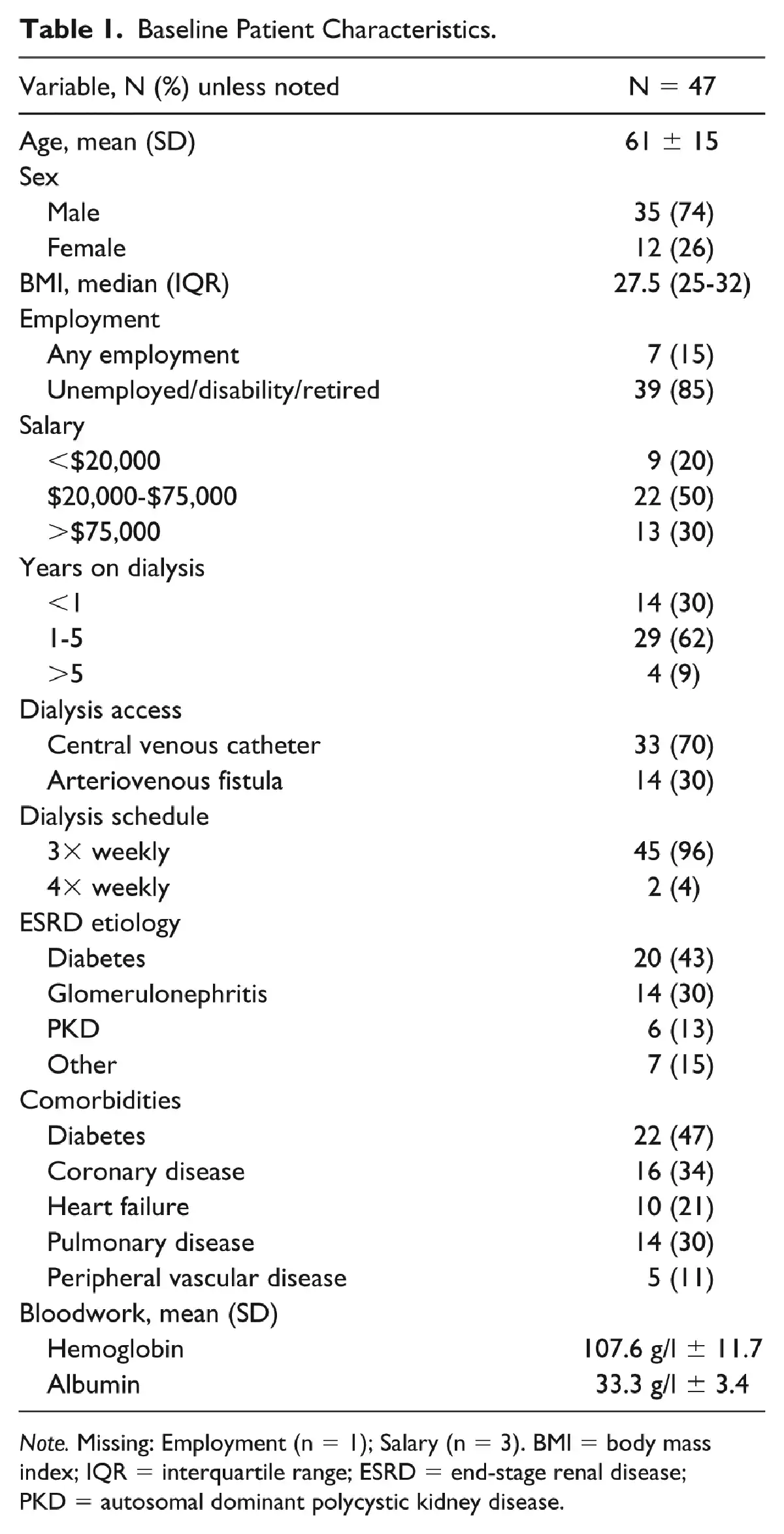
A total of 50 patients consented to participate in the study, 3 of whom withdrew (Figure 1). Baseline characteristics of the remaining 47 patients are noted in Table 1. The majority of our cohort was male (74%) and the mean age was 61 ± 15 years. Seventy-one percent of our cohort had been on dialysis for >1 year. A central venous catheter was the most common dialysis access. The most common cause of end-stage renal disease was diabetic nephropathy (43%), followed by glomerulonephritis (30%) and polycystic kidney disease (13%).
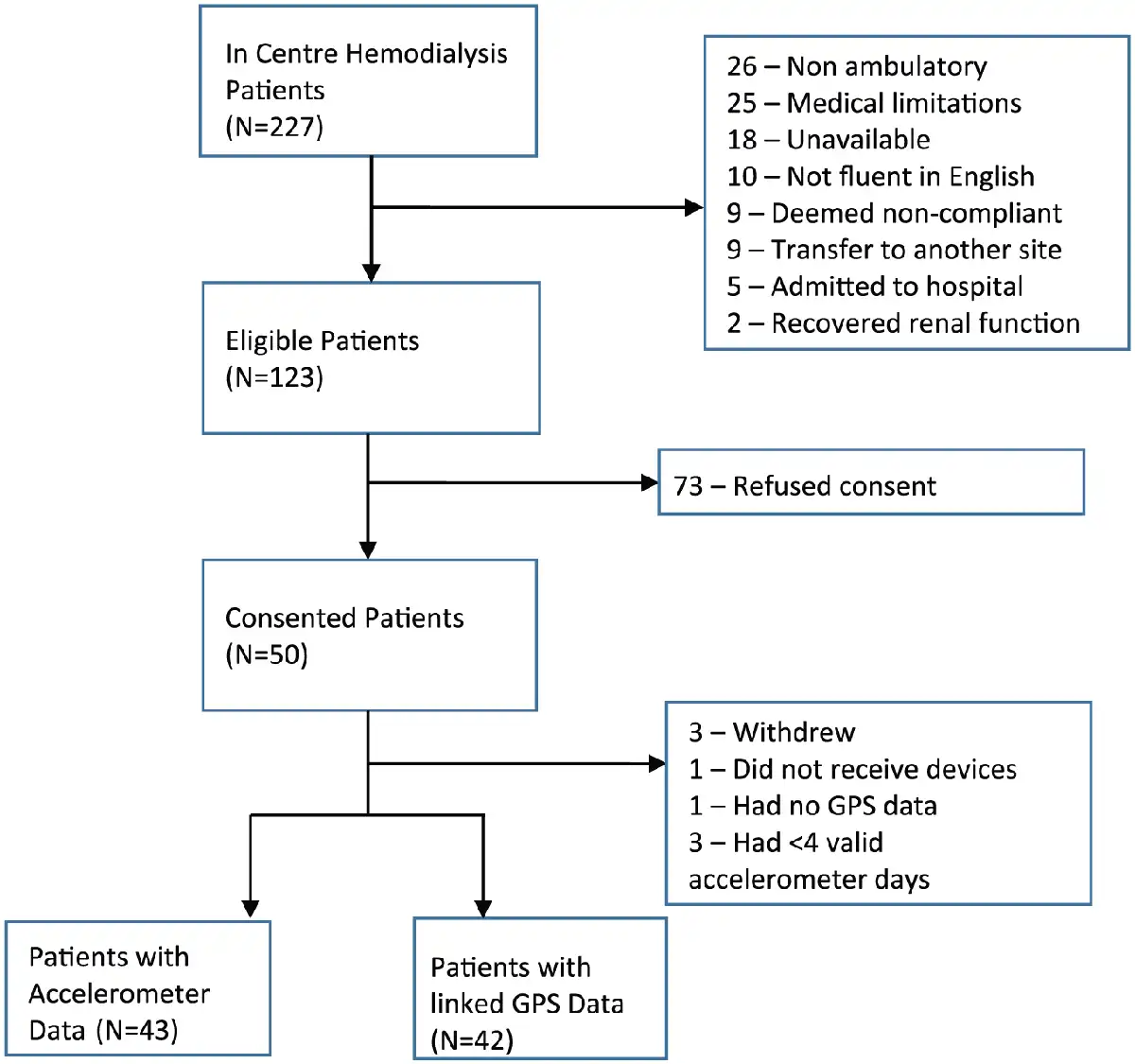
Figure 1
Flow chart depicting final study populations.
Note. GPS = global positioning system.
Accelerometer Data
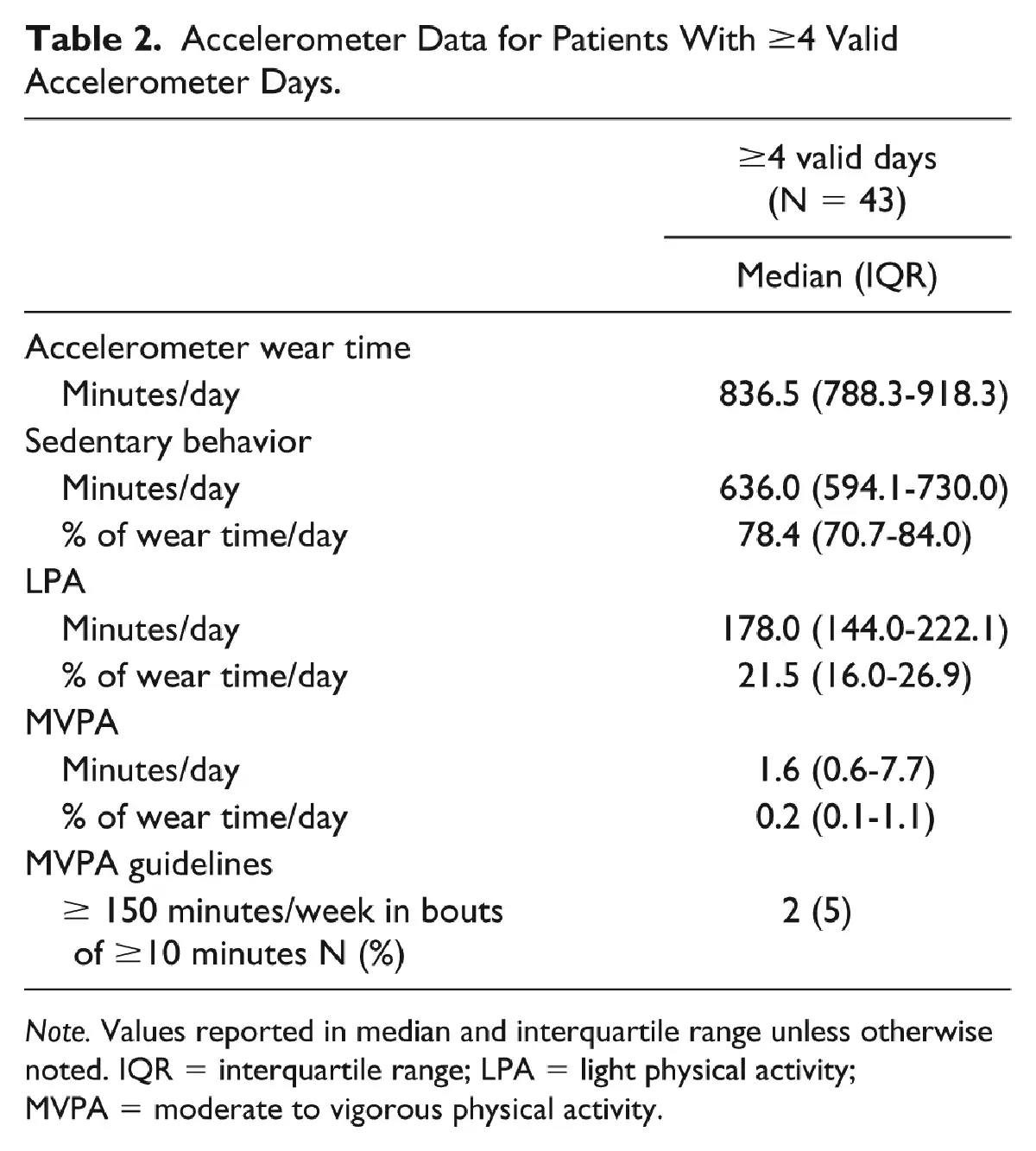
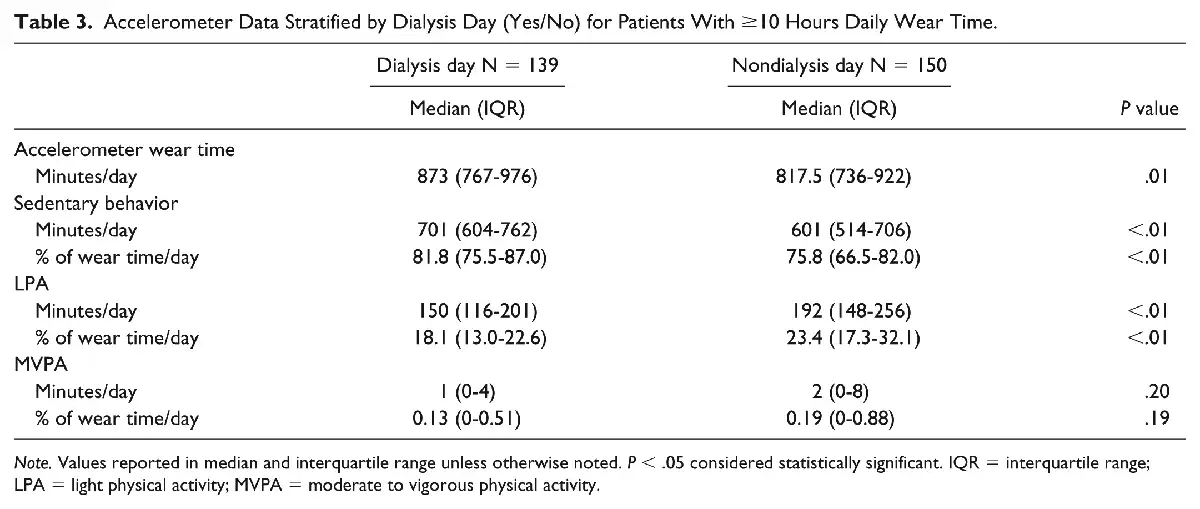
Of the 47 consenting patients, 1 did not receive the device (Figure 1). A total of 43 of 46 patients obtained 4 or more valid accelerometer days. The median accelerometer wear time was 836.5 min/day (interquartile range [IQR]: 788.3-918.3) equating to approximately 14 hours of daily wear time. In those with ≥4 valid accelerometer days, 636 min/day was spent sedentary (IQR: 594.1-730.0), 178 min/day was spent performing light physical activity (IQR: 144.0-222.1), and 1.6 min/day was spent on moderate to vigorous physical activity (IQR: 0.6-7.7) (Table 2). Only 2 people met the Canadian physical activity guidelines recommending ≥150 min/week of moderate to vigorous physical activity obtained in bouts of ≥10 minutes. Of the 289 individual valid accelerometer days, 139 occurred on a dialysis day and 150 on a nondialysis day. Comparisons of total daily minutes and proportion of daily time spent in each activity state for dialysis and nondialysis days are noted in Table 3. There was significantly less sedentary behavior on nondialysis days compared with dialysis days (601 min/day, IQR: 514-706; 701 min/day, IQR: 604-762; P ≤ .01) and more light physical activity (192 min/day, IQR: 148-256; 150 min/day, IQR: 116-201; P ≤ .01). Daily moderate to vigorous physical activity did not differ significantly between nondialysis and dialysis days (2 min/day, IQR: 0-8; 1 min/day, IQR: 0-4; P = .2).
Global Positioning System Data
Of the 47 consenting patients, 1 did not receive a GPS device and 1 did not collect any GPS data leaving an eligible cohort of 42 patients with linkable GPS data (using a cut-off of ≥4 valid accelerometer days; Figure 1). The percent of accelerometer data linked to GPS for sedentary behavior, light physical activity, and moderate to vigorous physical activity was 92.9%, 92.8%, and 97.5%, respectively. Five patients had no moderate to vigorous physical activity linked to GPS data and the median moderate to vigorous physical activity was 0.8 min/day in this group. The proportion of overall accelerometer use, sedentary behavior, light physical activity, and moderate to vigorous physical activity time for each coded GPS location is noted in Table 4. The majority of accelerometer wear time occurred in the home followed by hospital and transport. Home was also the dominant category across all levels of physical activity. Median percentage of sedentary behavior, light physical activity, and moderate to vigorous physical activity time in the home environment was 57.7%, 63.3%, and 60.3%, respectively. Hospital was the next most common location for sedentary behavior accounting for 17.8% of total sedentary time, whereas hospital and transportation were similar for light physical activity and moderate to vigorous physical activity. Minimal moderate to vigorous physical activity occurred outside of the home. The percent of daily linked time at a given location for different activity levels stratified by dialysis days can be seen in Supplementary Table 1. On dialysis days, there was significantly more daily sedentary time spent in the hospital compared with nondialysis days (36.2% vs 0%; P ≤ .001), whereas more sedentary time occurred at home on nondialysis days compared with dialysis days (76.6% vs 44.4% P ≤ .001). A summary of accelerometer and GPS findings is shown in Figure 2.
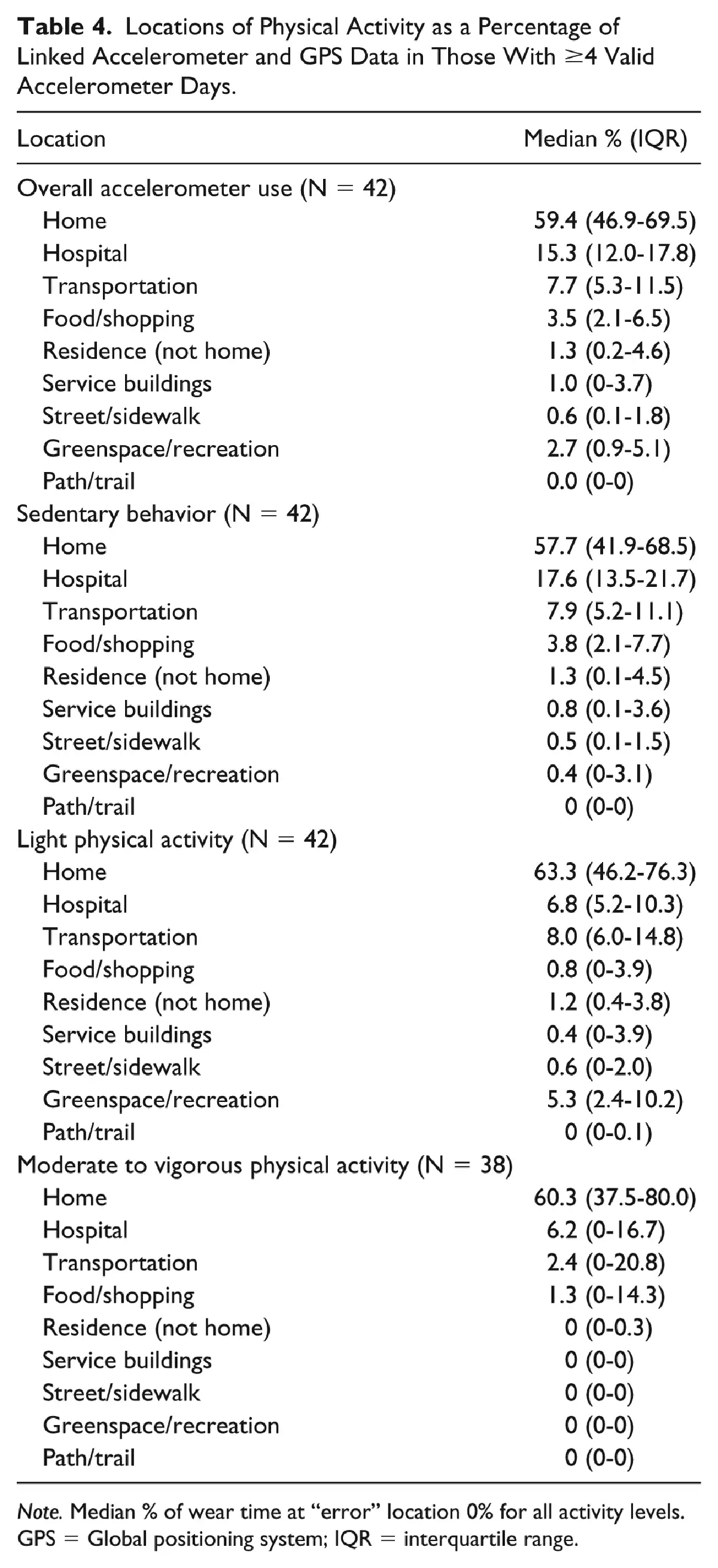
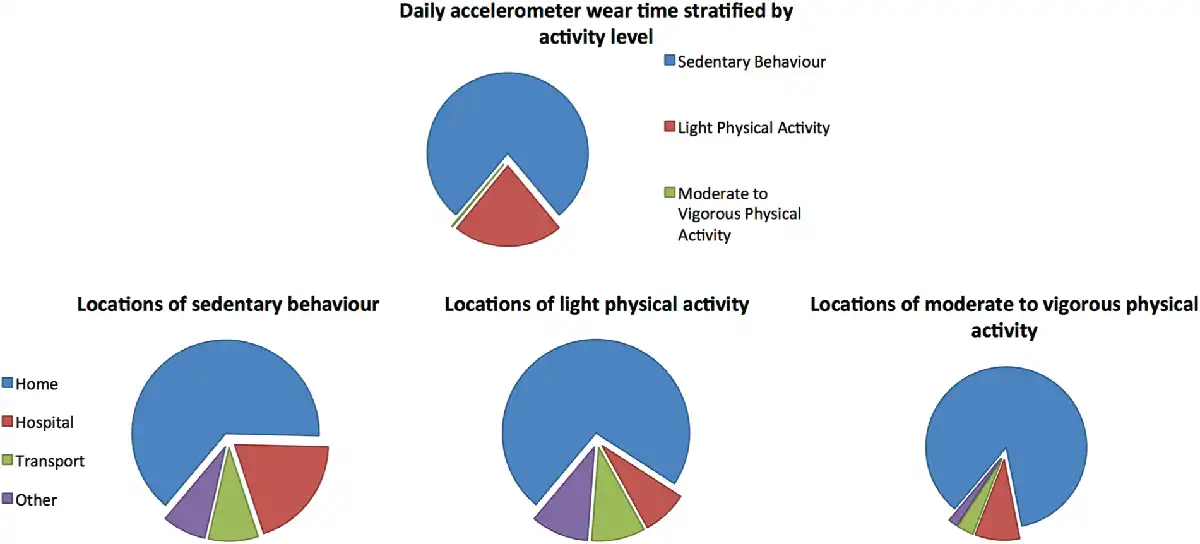
Figure 2
Daily accelerometer wear time stratified by activity level and locations where each activity level occurred.
Note. Exact proportions were not included as all values were medians.
Discussion
In this study, we linked accelerometer and GPS data to describe physical activity, sedentary behavior, and where these activities occur in a cohort of ambulatory, in-center hemodialysis patients. We found that hemodialysis patients exhibit minimal moderate to vigorous physical activity and substantial sedentary behavior. Furthermore, we found that irrespective of activity level, all behaviors seemed to occur across a limited range of locations including home, transportation, and hospital. Finally, we found differences in the types and locations of activity when comparing dialysis with nondialysis days; the proportion of time spent in a sedentary state was significantly higher on dialysis days compared with nondialysis days.
Our findings that dialysis patients exhibit minimal moderate to vigorous physical activity are consistent with other accelerometer-based studies of dialysis patients including a recent study which found that hemodialysis patients did on average only 5.7 minutes of moderate to vigorous physical activity per day. Only 4% of our study participants met the Canadian physical activity guidelines recommending ≥ 150 min/week of moderate to vigorous physical activity. This value is substantially lower than a recent Brazilian study which reported 35% of their hemodialysis cohort was able to achieve ≥ 150 min/week of moderate to vigorous physical activity. The discrepancy in these values is likely a result of following Canadian guidelines requiring moderate to vigorous physical activity to be acquired in bouts of ≥10 minutes, whereas the Brazilian study summed moderate to vigorous physical activity of any duration in patients who did on average <15 min/day of moderate to vigorous physical activity.
There are considerably fewer studies regarding objective assessment of sedentary behavior in hemodialysis patients. A previous study using pedometers and minimum steps per day demonstrated increased sedentary behavior in hemodialysis patients. Other studies have used accelerometers to show that hemodialysis patients are more sedentary than age- and sex-matched controls, and kidney transplant recipients based on daily step count. While informative, a limitation of these studies is that they defined sedentary behavior using a threshold of <5000 steps/day. This method dichotomizes sedentary behavior without capturing other important details such as total time and percentage of device wear time spent in a sedentary state. A recently published cross-sectional analysis describing accelerometer-measured sedentary time in the Canadian population showed sedentary behavior increased as estimated glomerular filtration rate (eGFR) declined and those in the lowest eGFR cohort (<45 mL/min/m2) spent upward of 80% of total wear time in a sedentary state. Although comparable, there are several possible reasons why the proportion of sedentary behavior time in our hemodialysis cohort was lower. First, our cohort was younger (61 vs 71 years) and may be more active. Second, our upper limit for defining sedentary behavior was 0.5 METs lower than the criteria used in the cross-sectional analysis. Thus, people who performed light physical activity in our study may be been classified as sedentary in the cross-sectional analysis. Third, prior studies have shown an association between male sex and increased physical activity and our cohort contained a higher percentage of male participants (74% vs 58%). Finally, our cohort was ambulatory and excluded individuals with forms of mobility impairment not limited to wheelchair dependence. We also found that hemodialysis patients exhibited more sedentary behavior and less light physical activity, and moderate to vigorous physical activity on dialysis days compared with nondialysis days, which is consistent with previous studies. This was not unexpected given the stationary time required for hemodialysis as well as postdialysis fatigue often reported by patients.
Sedentary behavior in our population is comparable with reported values in other frail populations. A study of sedentary behavior in a cohort of community dwelling adults ≥65 years old who were 3 to 12 months post hip fracture showed that up to 77% of daily accelerometer wear time was spent sedentary. Another study involving patients beginning cardiac rehabilitation found that 71% of daily accelerometer wear time was spent in a sedentary state. Both of these populations are also burdened by comorbidity and frailty, similar to in-center hemodialysis patients.
Studies have shown an association between sedentary behavior and all-cause mortality using objective accelerometer data in the general population. In dialysis, sedentary behavior is also associated with an adjusted increased risk of death at 1 year (HR: 1.62; 95% CI: 1.16-2.27). These studies illustrate the implications of sedentary behavior and, in concert with the high prevalence of sedentary behavior in our study, potentially underscore the need for future studies focusing on reducing sedentary behavior in hemodialysis patients.
To our knowledge, linking physical activity to real-world locations using objective GPS data has not been done in this population. Locations obtained with GPS methodology should be more accurate than subjective questionnaire-based location assessments. A striking finding from our GPS data is the extensive proportion of time spent at home across all activity levels. While the majority of moderate to vigorous physical activity occurred in the home environment, the total minutes per day of moderate to vigorous physical activity was minimal. Thus, it may prove prudent to focus on any location to increase moderate to vigorous physical activity given how little is done overall. Potential benefits of increasing moderate to vigorous physical activity outside of the home environment include prevention of social isolation and strengthen support networks which may help with exercise sustainability.
The vast majority of sedentary behavior occurred in the home environment followed by the hospital and transportation. Appreciating that both time in hospital and transportation was higher on dialysis days, we suspect the high proportion of sedentary behavior in these locations was directly related to the hemodialysis treatment. Breaking up sedentary time during hemodialysis using intradialytic exercise programs has been shown to have numerous benefits. While these strategies are useful for dialysis days, they do not directly address sedentary behavior occurring on nondialysis days. Interventions focused on reducing sedentary behavior in the home environment may provide additional benefit due to the large amount of time this population spends at home. A recent randomized controlled trial showed that a home-based walking exercise program was able to significantly increase physical performance in dialysis patients at 6 months compared with normal daily activity. Home-based programs such as this should be seen as complimentary to intradialytic therapies and would help to interrupt sedentary behavior at home, given the amount of time per day spent in this location irrespective of dialysis or nondialysis day.
This study has a number of strengths. First, using accelerometers allowed us to objectively capture descriptive details of physical activity and sedentary behavior including intensity and duration. We chose an MET/count-based definition of sedentary behavior which more accurately describes sedentary behavior compared with steps/day. Finally, using GPS to describe locations of moderate to vigorous physical activity, light physical activity, and sedentary behavior in the hemodialysis population has not previously been done to our knowledge. Limitations of our study include a small sample size from a single center, and a cross-sectional design that does not allow participants to be followed over time. Our study highlights the difficulty with recruiting and engaging the hemodialysis population as less than half of eligible patients provided consent. A control group was not included as our study was cross-sectional; however, physical activity in the general population has been well described. Participants may have increased their activity while wearing the accelerometer, but it is unlikely this contributed in a meaningful fashion and would have led to an underestimate of an already substantial sedentary time. Finally, activity levels may have been underestimated as devices were not worn for all awake hours, the hip-based accelerometer location may not capture stationary exercise (eg, cycling), and devices were removed before water-based activity as they were not waterproof.
Conclusion
Ambulatory, in-center hemodialysis patients demonstrate minimal moderate to vigorous physical activity and significant sedentary behavior across a limited range of locations. Given the substantial sedentary tendencies of this population, focus should be directed on increasing physical activity at any location frequented. Home-based exercise programs may serve as a potential adjunct to intradialytic-based therapies given the amount of time spent in the home environment.
This study was presented in poster format at the American Society of Nephrology Kidney Week in San Diego, California, on October 26, 2018.
Ethics Approval and Consent to Participate The Nova Scotia Health Authority Research Ethics Board (#1022204) approved this study. All participants provided written informed consent.
Consent for Publication All authors have provided consent for publication.
Availability of Data and Materials Data and materials are available upon request by contacting the corresponding author Dr. Karthik Tennankore.
Declaration of Conflicting Interests The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported through the Nova Scotia Health Authority Research Fund Competition.
Keigan M. More
https://orcid.org/0000-0003-4903-6680
Supplemental Material Supplemental material for this article is available online.
References
- 1. Johansen KL, Chertow GM, Ng AV, et al. Physical activity levels in patients on hemodialysis and healthy sedentary controls. Kidney Int. 2000;57(6):2564–2570. doi:.
- 2. Gomes EP, Reboredo MM, Carvalho EV, et al. Physical activity in hemodialysis patients measured by triaxial accelerometer. Biomed Res Int. 2015;2015:645645. doi:.
- 3. Lopes AA, Lantz B, Morgenstern H, et al. Associations of self-reported physical activity types and levels with quality of life, depression symptoms, and mortality in hemodialysis patients: the DOPPS. Clin J Am Soc Nephrol. 2014;9(10):1702–1712. doi:.
- 4. Stack AG, Molony DA, Rives T, Tyson J, Murthy BV. Association of physical activity with mortality in the US dialysis population. Am J Kidney Dis. 2005;45(4):690–701.
- 5. O’Hare AM, Tawney K, Bacchetti P, Johansen KL. Decreased survival among sedentary patients undergoing dialysis: results from the dialysis morbidity and mortality study wave 2. Am J Kidney Dis. 2003;41(2):447–454. doi:.
- 6. Johansen KL, Kaysen GA, Dalrymple LS, et al. Association of physical activity with survival among ambulatory patients on dialysis: the comprehensive dialysis study. Clin J Am Soc Nephrol. 2013;8(2):248–253. doi:.
- 7. Matsuzawa R, Matsunaga A, Wang G, et al. Habitual physical activity measured by accelerometer and survival in maintenance hemodialysis patients. Clin J Am Soc Nephrol. 2012;7(12):2010–2016. doi:.
- 8. Matsuzawa R, Roshanravan B, Shimoda T, et al. Physical activity dose for hemodialysis patients: where to begin? results from a prospective cohort study. J Ren Nutr. 2018;28(1):45–53. doi:.
- 9. Rosa CS, Gracia-Marco L, Barker AR, Freitas IF Jr, Monteiro HL. Assessment of physical activity by accelerometer and IPAQ-short version in patients with chronic kidney disease undergoing hemodialysis. Blood Purif. 2015;40(3):250–255. doi:.
- 10. Majchrzak KM, Pupim LB, Chen K, et al. Physical activity patterns in chronic hemodialysis patients: comparison of dialysis and nondialysis days. J Ren Nutr. 2005;15(2):217–224.
- 11. da Costa Rosa CS, Nishimoto DY, Freitas IF Jr, Ciolac EG, Monteiro HL. Factors associated with levels of physical activity in chronic kidney disease patients undergoing hemodialysis: the role of dialysis versus nondialysis day. J Phys Act Health. 2017;14(9):726–732. doi:.
- 12. Carvalho EV, Reboredo MM, Gomes EP, et al. Physical activity in daily life assessed by an accelerometer in kidney transplant recipients and hemodialysis patients. Transplant Proc. 2014;46(6):1713–1717. doi:.
- 13. Grontved A, Hu FB. Television viewing and risk of type 2 diabetes, cardiovascular disease, and all-cause mortality: a meta-analysis. JAMA. 2011;305(23):2448–2455. doi:.
- 14. Hurvitz PM, Moudon AV, Kang B, Fesinmeyer MD, Saelens BE. How far from home? the locations of physical activity in an urban U.S. Prev Med. 2014;69:181–186. doi:.
- 15. Holliday KM, Howard AG, Emch M, Rodriguez DA, Rosamond WD, Evenson KR. Where are adults active? an examination of physical activity locations using GPS in five US cities. J Urban Health. 2017;94(4):459–469. doi:.
- 16. Johansen KL, Chertow GM, Jin C, et al. Significance of frailty among dialysis patients. J Am Soc Nephrol. 2007;18:2960–2967. doi:.
- 17. Metcalf BS, Curnow JS, Evans C, Voss LD, Wilkin TJ. Technical reliability of the CSA activity monitor: The EarlyBird Study. Med Sci Sports Exerc. 2002;34(9):1533–1537. doi:.
- 18. Welk GJ, Schaben JA, Morrow JR Jr. Reliability of accelerometry-based activity monitors: a generalizability study. Med Sci Sports Exerc. 2004;36(9):1637–1645.
- 19. Choi L, Liu Z, Matthews CE, Buchowski MS. Validation of accelerometer wear and nonwear time classification algorithm. Med Sci Sports Exerc. 2011;43(2):357–364. doi:.
- 20. Troiano RP, Berrigan D, Dodd KW, et al. Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc. 2008;40:181–188. doi:.
- 21. Rodríguez DA, Shay E, Winn P. Comparative review of portable global positioning system units. In: Hsueh Y, ed. Global Positioning Systems: Signal Structure, Applications and Sources of Error and Biases. New York, NY: Nova Science; 2013:1–16.
- 22. Tremblay MS, Warburton DE, Janssen I, et al. New Canadian physical activity guidelines. Appl Physiol Nutr Metab. 2011;36:36–46;47-58. doi:.
- 23. Colley RC, Garriguet D, Janssen I, Craig CL, Clarke J, Tremblay MS. Physical activity of Canadian adults: accelerometer results from the 2007 to 2009 Canadian Health Measures Survey. http://www.statcan.gc.ca/pub/82-003-x/2011001/article/11396-eng.htm. Published 2010. Accessed April 24, 2017.
- 24. Cobo G, Gallar P, Gama-Axelsson T, et al. Clinical determinants of reduced physical activity in hemodialysis and peritoneal dialysis patients. J Nephrol. 2015;28:503–510. doi:.
- 25. Glavinovic T, Ferguson T, Komenda P, et al. CKD and sedentary time: results from the Canadian health measures survey. Am J Kidney Dis. 2018;72:529–537. doi:.
- 26. Bossola M, Tazza L. Postdialysis fatigue: a frequent and debilitating symptom. Semin Dial. 2016;29:222–227. doi:.
- 27. Zusman EZ, Dawes M, Fleig L, et al. Older adults’ sedentary behavior and physical activity after hip fracture: results from an outpatient rehabilitation randomized controlled trial. J Geriatr Phys Ther. 2019;42(2):E32–E38. doi:.
- 28. Ramadi A, Haennel RG. Sedentary behavior and physical activity in cardiac rehabilitation participants. Heart Lung. 2019;48:8–12. doi:.
- 29. Schmid D, Ricci C, Leitzmann MF. Associations of objectively assessed physical activity and sedentary time with all-cause mortality in US adults: the NHANES study. PLoS One. 2015;10:e0119591. doi:.
- 30. Sheng K, Zhang P, Chen L, et al. Intradialytic exercise in hemodialysis patients: a systematic review and meta-analysis. Am J Nephrol. 2014;40:478–490. doi:.
- 31. Manfredini F, Mallamaci F, D’Arrigo G, et al. Exercise in patients on dialysis: a multicenter, randomized clinical trial. J Am Soc Nephrol. 2017;28:1259–1268. doi:.