Introduction
Mental disorders are a major contributor to the global burden of disease (GBD) (GBD 2019 Mental Disorders Collaborators, ). They also affect most dimensions of human life, having a high level of social stigmatization (Patel et al., ). The case for more investment in mental health has long been made, and mental healthcare expenditure has increased significantly, at least in many wealthy countries (Christensen et al., ). The World Health Organization (WHO) has also argued that the importance of investing more resources into mental healthis also about additional impacts on physical health; for example, people living with major depression or schizophrenia have a 40%–60% greater chance of premature mortality compared to people without mental disorders (World Health Organization, ).
The attention given to mental health in high-income countries may, in part, reflect data indicating that the prevalence and number of disability-adjusted life years (DALYs) attributable to mental disorders are much higher in high-income countries, i.e. in countries classified by the World Bank in 2024–2025 as having a gross national income (GNI) per capita of more than $14,005, compared with lower-middle income countries with GNI per capita between $1,146 and $4,515 or low-income countries with a GNI per capita of less than $1,146 per capita (Metreau et al., ).
One caveat, however, is that the GBD burden in low- and lower-middle-income countries in sub-Saharan Africa varies substantially, so there is considerable uncertainty around differences in GBD between countries because of limited epidemiological data in Africa (Omigbodun et al., ). Countries in the lowest income categories are less likely to ensure a minimal level of medical treatment or psychosocial care for those with the most severe mental illnesses (OECD, ; World Health Organization, ). The mean number of psychiatric hospital beds per 100,000 population in 2017 was only 1.9 in low-income countries, in contrast to 28.6 in high-income countries (World Health Organization, ).
Given that international action plans recommend a shift in the care balance from hospital to community-based care (World Health Organization, ), as well as integrating mental health into primary care in low- and middle-income countries (Thornicroft and Tansella, ), these disparities are even more stark. There are 30 community mental health outpatient visits per 100,000 population in low-income countries, in contrast to about 3,000 in high-income countries (World Health Organization, ). In addition to disparities between high- and low-income countries, there are also large differences between countries within the same income categories in terms of performance against mental healthcare targets, as defined by the WHO Comprehensive Mental Health Action Plan and OECD mental health benchmark indicators (OECD, ; World Health Organization, ).
To date, most comparisons on mental health service use have been based on aggregate-level top-down data or expert surveys (Arias et al., ; Rajkumar, ). Individual patient-level data are rarely available (Addo et al., ). These data tend to give the overall impression of a lack of mental healthcare resources and infrastructure. However, they do not reveal how people with mental health problems make use of available services or the extent to which the lack of professional mental healthcare can be compensated by social support or other types of informal healthcare, such as traditional healers (Mokgobi, ).
Our study aims to compare total costs of illness (COIs) in people living with mental disorders in a standardized way across five countries – covering three of the four categories of the World Bank income scale: Germany and Israel (high income), India and Tanzania (lower middle income) and Uganda (low income). The countries provide a spectrum of policy and practice contexts. The two high-income countries are examples of different approaches to the management of mental disorders. Reform in Israel in 2015 moved responsibility for mental health from the Ministry of Health to four social health insurers with the aim of integrating mental health into general health services with more focus on community-based care (Gal et al., ). In contrast, the German system has not experienced this transformation and has continued to operate a model dominated by psychiatric inpatient care and less integration with community services (Wiegand et al., ). Indian national mental health policy, coupled with reforms to expand access to publicly funded healthcare, has put a focus on community mental health services (Mahapatra and Seshadri, ). Uganda has had a national mental health policy for almost 30 years, which also commits to more community-focused care (Atewologun et al., ), while Tanzania represents a country with little history of mental health policy development (Atewologun et al., ).
Our study explores whether total COIs are associated with diagnosis, socio-demographic characteristics and Health of the Nation Outcome Scale (HoNOS) scores. It looks at differences in patterns in service utilization, using bottom-up costing methods (Knapp and Beecham, ), with individual health service user data. Results are primarily expected to provide insights into the effects of economic disparities on mental health service use and secondarily to have implications for improvement strategies.
Methods
Contextual information on country characteristics was taken from published literature, including gross domestic product (GDP) per capita (World Bank, ), total governmental health expenditure as a percentage of GDP and proportion of expenditure allocated to mental health (GBD 2019 Mental Disorders Collaborators, ). Funding structures and mental health service capacity were taken from the WHO Mental Health Atlas’ 2020 (Germany, Tanzania and Uganda) (World Health Organization, ) and 2017 (India and Israel) (Jaeschke et al., ).
The investigation makes use of baseline data from the ‘Using Peer Support In Developing Empowering Mental Health Services (UPSIDES)’ study (Moran et al., ). UPSIDES is an international multisite trial, assessing the effectiveness of implementing peer support for people with severe mental illness in these five countries.
Study sample
Participants aged 18–60 years were recruited at psychiatric treatment facilities. Detailed information on study sites and recruitment strategies is found in the study protocol; they included multiple strategies, including ‘outpatient/community mental health services, patient/carer organisations, local newspapers, social media, community leaders, and word of mouth’ (Moran et al., ).
Participants needed a mental disorder diagnosis according to case notes, staff communication or self-labelling for at least 24 months, as well as a severity-of-illness threshold of 5 points or more assessed using the Threshold Assessment Grid, with illness duration (2 years and over) (Slade et al., ). Additionally, participants needed to have the capacity to provide written informed consent in their local language. Exclusion criteria included learning disability, dementia, substance disorder or organic brain disorder diagnoses. Social disability was measured using the HoNOS (score ranges: 0–48, higher scores indicating greater severity) (Wing et al., , ).
Assessment of healthcare use
Use of medical and psychosocial services and support was comprehensively assessed using the Client Sociodemographic and Service Receipt Inventory (CSSRI) (Chisholm et al., ), adapted for use in participating countries as the CSSRI-UPSIDES (Charles et al., ). For adaptation purposes, mental healthcare experts from participating study sites were consulted to check service categories of the original instrument for applicability and to add and define country or site-specific services or support categories not already included (Moran et al., ).
The main categories of CSSRI-UPSIDES are all inpatient and outpatient health services, community mental health services, primary healthcare, justice system services, medication and out-of-pocket payments. Inpatient services include all types of inpatient hospital treatment; outpatient services include all types of outpatient treatment provided by hospitals or by office-based physicians; and community mental health services include psychosocial services provided in the community, such as in day centres, occupational rehabilitation and housing support. Primary healthcare services include all medical services provided in the community free of charge, such as family doctors, community health centres, community nurses and midwives. Justice includes costs for police contacts, detention, time in police custody, imprisonment and trials. Costs for medication cover those taken outside of hospital settings.
Collection of unit cost information
Country-specific costs for service units were obtained from publicly available sources and consultation with mental health service experts at study sites (see Supplementary eTables 1–5, Supplement 1, for country values). For potential reliability issues, unit costs were triangulated using published information, expert communications and communications with local facility staff members. Due to the unavailability of reliable country-specific cost information for all countries, drug costs were calculated on the basis of the British National Health Service Drug Tariff (National Health Service Business Service Authority (NHSBSA), ).
Estimation of the total cost of illness
Reported service units were multiplied by unit costs in the local currency. Costs for outpatient care over 3 months and costs for medical drugs for 1 month were extrapolated to estimate costs for a 6-month period. To allow comparison, all country-specific costs were converted to one currency (2021 price years), expressed as international dollars (Int$), using purchasing power parity (PPP) (International Monetary Fund, ). All relevant elements of the Consolidated Health Economic Evaluation Reporting Standards 2022 (CHEERS 2022) Statement (Husereau et al., ) were followed (Supplement 2).
Statistical analysis
Generalized linear models (GLMs) with log link and gamma distribution of errors were applied to account for skewed distribution of healthcare cost data (Kilian et al., ; Mccullagh, ). Initially, country-specific models were estimated with gender, age, psychiatric diagnosis and HoNOS total score as independent variables. Subsequently, an overall model was computed including dummy variables for country using Germany as a reference category. To account for country-specific differences, multiplicative interaction terms between country × gender, country × age, country × diagnosis and country × HoNOS were included. To facilitate interpretation, regression coefficients were reported as exponentiated betas. Since the GLM provides no R2 statistic, we computed R2 from the correlation between raw costs (y) and costs predicted by the regression equation
as
2. Diagnostic residual plots were produced to test model requirements. Statistical analyses were conducted in Stata 17 (StataCorp, ).
The study was approved by the Ethics Commission of Ulm University, Germany (ref. 254/19), Local Psychological Ethics Commission, Center for Psychological Medicine, Hamburg, Germany (ref. LPEK-0095), Uganda National Council for Science and Technology (ref. SS 4990), National Institute for Medical Research, Das es Salaam, and Ministry of Health, Community Development, Gender, Elderly & Children, Dodoma, Tanzania (ref. NIMR/HQ/R.8a/Vol.IX/3328), the Human Subjects Research Committee of Ben-Gurion University, Israel (ref. 1878-1) and the Indian Law Society (ref. LIS/37/2018).
Results
Table 1 provides information on country characteristics. GDP per capita ranged from $2,275 in Uganda to $54,551 in Germany, a 24-fold difference. GDP percentage spent on overall healthcare varied from 2.96% in India to 13% in Germany. Mental health expenditure as a percentage of the total health expenditure ranged from 1.3% in India to 13.1% in Germany. Mental healthcare in Germany and Israel was mainly funded by statutory health insurance, with 90% and 95% coverage, respectively. That said, 3.4% overall spending on mental health in Israel as a proportion of total governmental health expenditure is similar to the three other countries in our analysis. However, India, Tanzania and Uganda relied predominantly on out-of-pocket payments and private health insurance schemes, while in Israel, mental health is covered by the statutory health system.
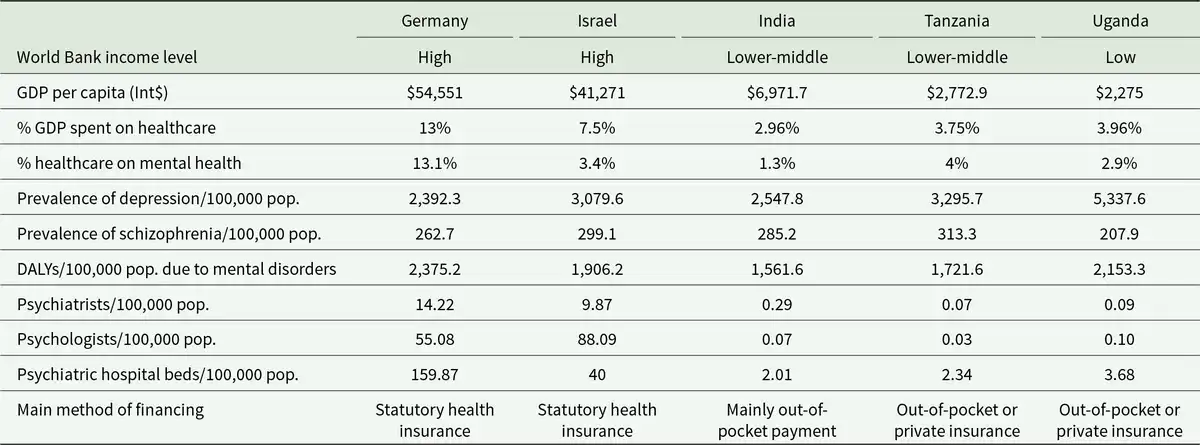
While prevalence rates for schizophrenia were similar among the five countries, the prevalence of depression per 100,000 population was highest at 5,337.6 in Uganda and lowest at 2,392.3 in Germany (GBD 2019 Mental Disorders Collaborators, ). Rates for DALYs per 100,000 population varied between 1,561.6 in India and 2,153.3 in Uganda (GBD 2019 Mental Disorders Collaborators, ).
Regarding workforce, the number of psychiatrists ranged from 0.06 per 100,000 population in Tanzania to 13 in Germany (World Health Organization, ). Israel had the highest number of psychologists per 100,000 population (88.09), while this ranged from 0.01 to 0.08 in lower-middle and low-income countries. Germany had the highest number of psychiatric hospital beds (150 per 100,000), followed by Israel (40), whereas very low rates were reported in the other countries (1.34–2.45).
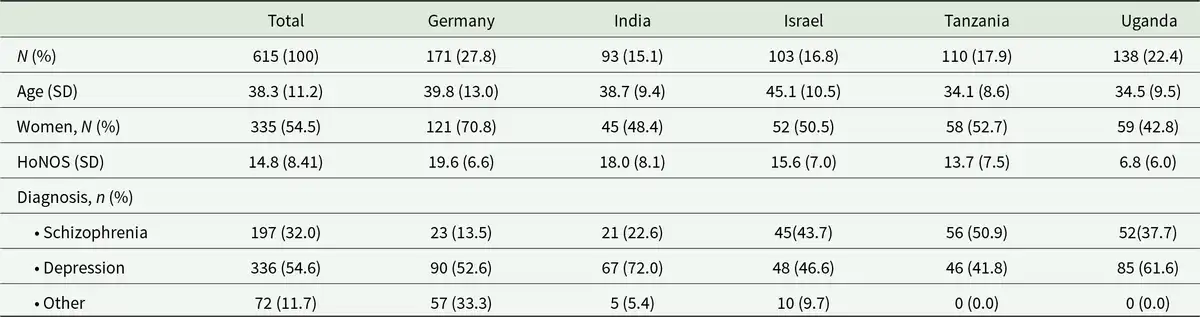
Baseline characteristics of all 615 participants are reported in Table 2. The mean age was 38.3 (SD 11.2 years), and the study was broadly balanced; 54.5% were women. The mean HONOS score was 14.8, ranging from 19.6 in Germany to 6.8 in Uganda. In total, 54% had a depression diagnosis.
Total costs for healthcare in five countries
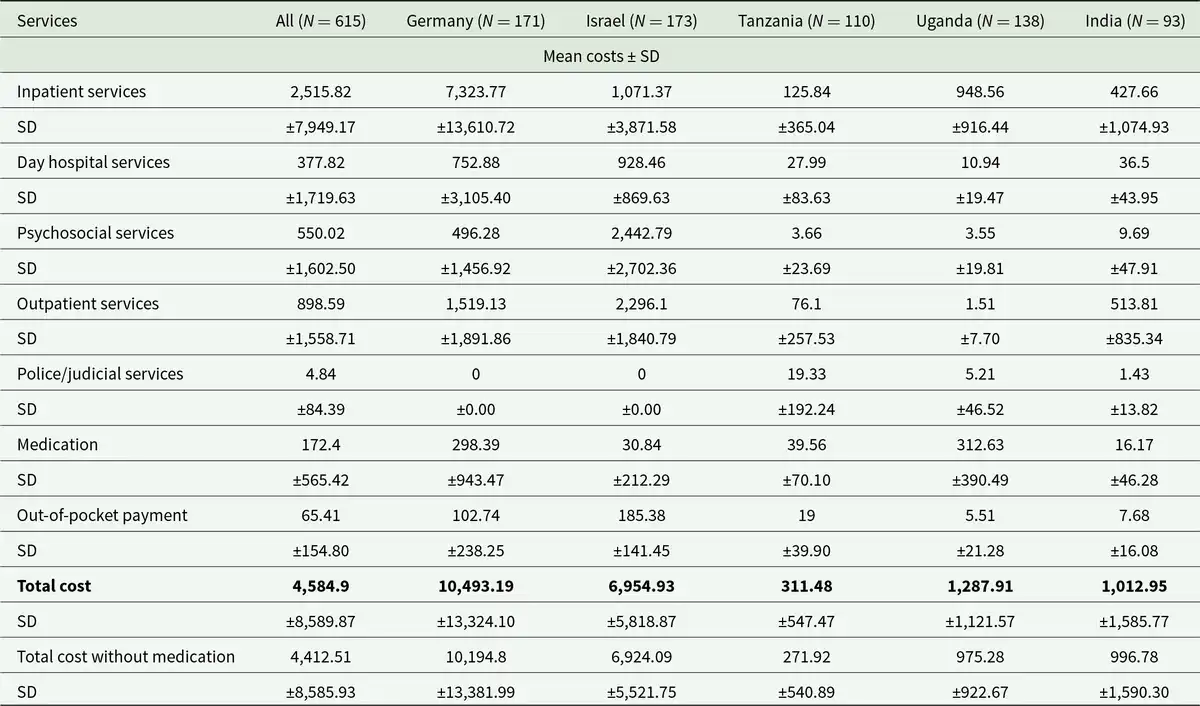
Table 3 shows total healthcare costs, disaggregated by cost component. Total costs ranged from $311.48 in Tanzania to $10,493.19 in Germany. Comparison of balance between different cost categories in Figure 1 indicates that 69.80% (Germany) and 73.65% (Uganda) of costs were for inpatient care. German respondents also reported 14.48%, 7.17% and 4.73% of expenditures were for primary, outpatient and community care. The almost complete reliance on inpatient care in Uganda, where the only other costs reported were for medications, coupled with the relatively low unit costs for inpatient care, meant a mean of more than 25 nights spent in hospital over the 6-month time period, much higher even than in Germany at almost 20 nights, because of the higher unit costs of care. Mean inpatient stays were approximately 13 nights in India, 3 in Israel and 2 in Tanzania.
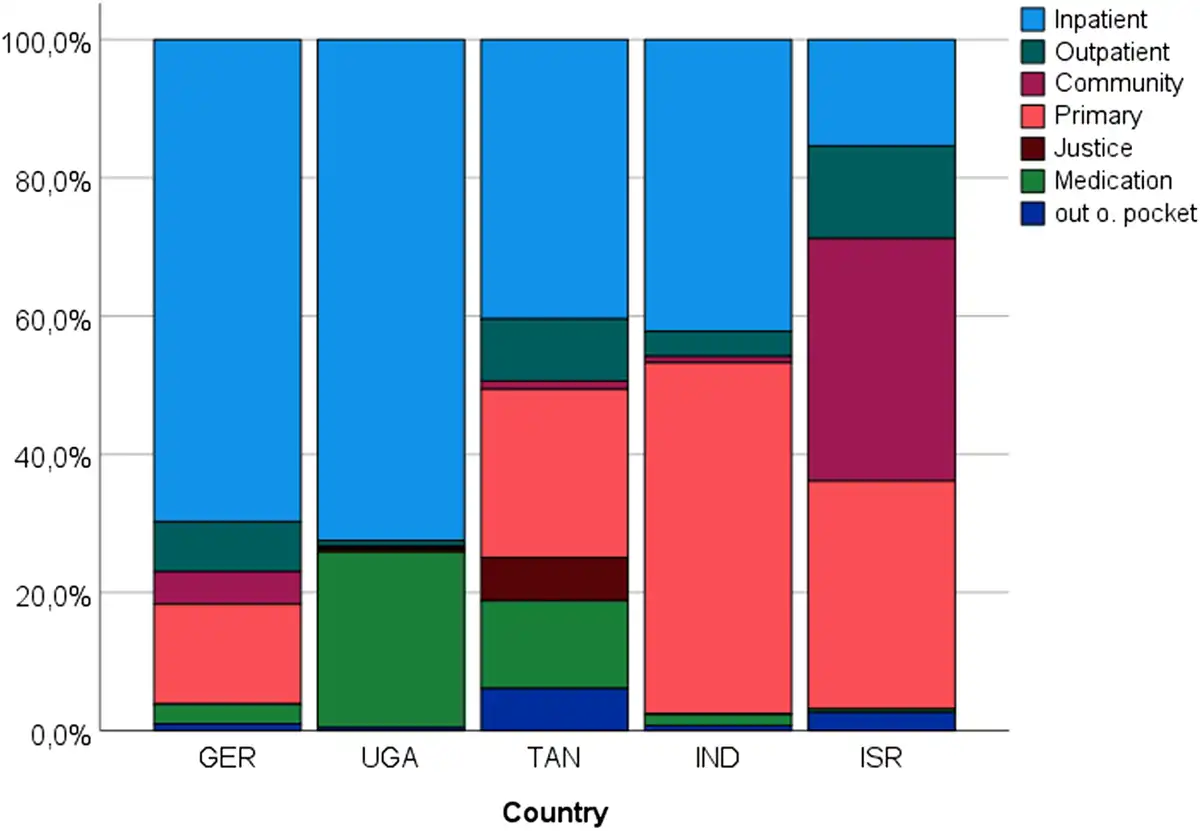
Figure 1
Distribution of total healthcare expenditure (GER = Germany; UGA = Uganda; TAN = Tanzania; IND = India; ISR = Israel).
Inpatient care as a share of total expenditure remained substantial in both Tanzania (40.40%) and India (42.22%), but primary care had the greatest share of costs in India (50.72%). Tanzanian respondents included the highest expenditures for the justice system (6.21%); this could reflect a lack of access to healthcare services. Israel spent the lowest proportion (15.40%) of resources on inpatient care, while remaining expenditures were distributed relatively equally between community (35.12%) and primary care (33.01%), with a lesser share for outpatient treatment (13.35%).
Relationships of factors with total costs
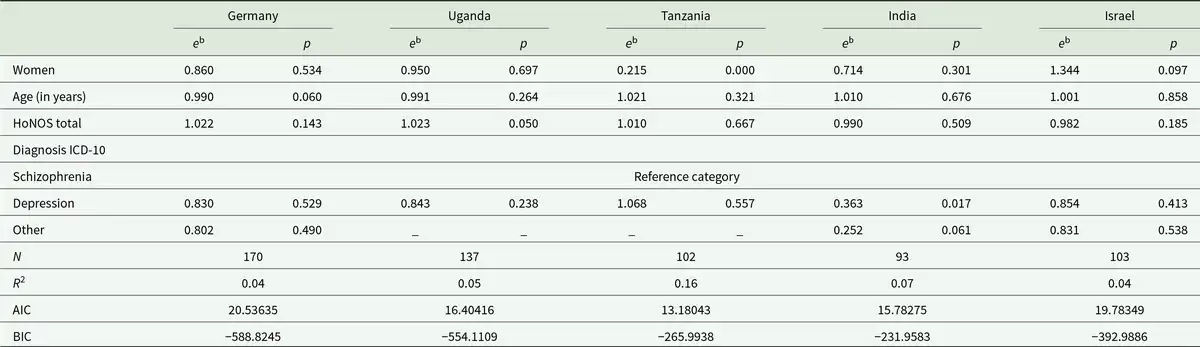
Results of country-specific GLM regression models in Table 4 show that gender was only significant in Tanzania where being a woman was associated with lower expenditure (eb = 0.215; p = 0.000). Diagnosis was only significantly associated with total mental health costs in India, where compared to schizophrenia, a diagnosis of depression was associated with lower expenditure (eb = 0.363; p = 0.017). Age and HoNOS scores (social disability) were not significantly associated with total costs in any country. The R2 of 0.16 indicates that 16% of the total cost variance could be explained by the variables in the regression model for Uganda, while the variance explanation for the other countries ranged between 4% and 7%. The residual plots in Supplementary eTables 1–5 indicate deviances from the requirement of normal distribution, particularly for the Tanzanian and for the Indian sample. While the Bayesian information criterion (BIC) suggests the best fit for the German model, the Akaike information criterion is lowest for the Tanzanian model. This indicates that the ratio between the sample size and the number of model variables is better in the German model.
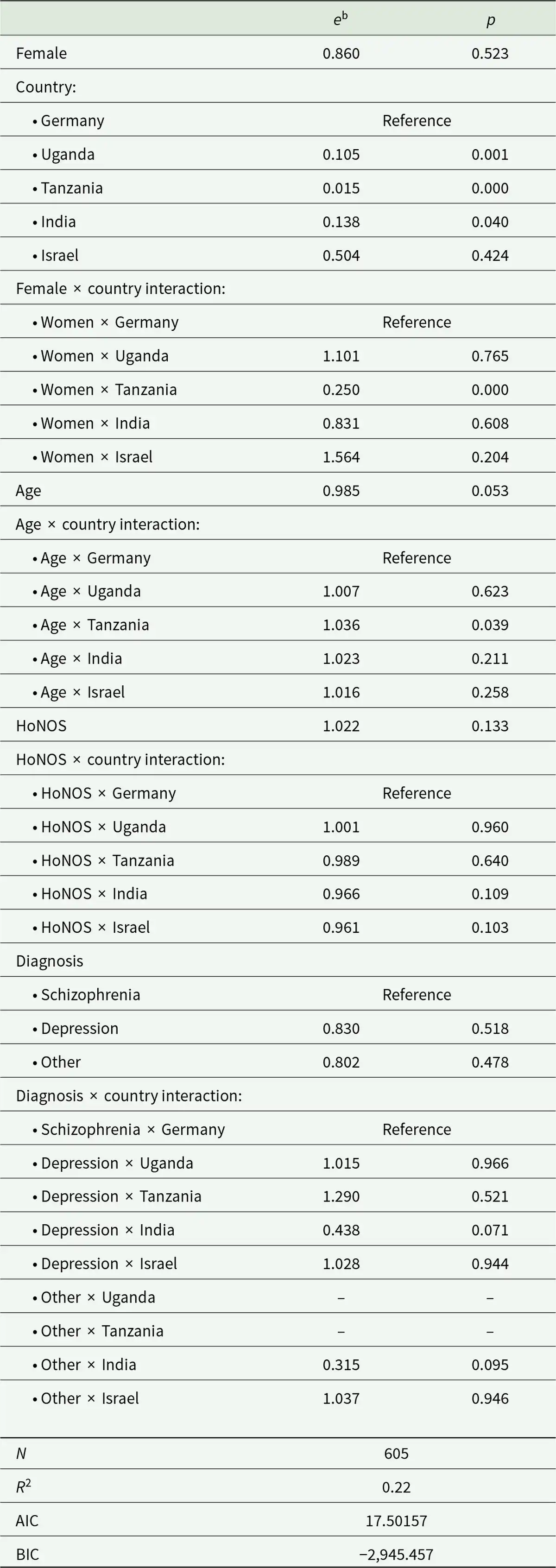
The results of the GLM regression on total costs across all countries in Table 5 indicate that compared to Germany, mean expenditure per participant was significantly lower in Uganda (90%), Tanzania (99%) and India (86%). Given the significant interaction effects between female gender and country, female gender in Tanzania was associated with a 75% reduction in the total mental health service costs, relative to the costs for women in Germany. Additionally, the significant coefficient for the age × country interaction indicates Tanzanian healthcare costs increased by 3.6% for every additional year of age. There were no other country interaction effects with age, HoNOS or diagnosis. The R2 of 0.22 indicates that the overall model explains 22% of the variance in the total COI. The positive AIC and the negative BIC indicate a good ratio between the sample size and the number of model variables. The distribution of the residuals in Supplementary eFigure 6 indicates no deviance from the normal distribution.
Discussion
While national income is correlated with the total COI in people living with mental disorders, it is a poor predictor of the sector-specific distribution of these expenditures and it can be argued that in these five settings, with vastly different systems, there is a need for more focus on primary care. Mean expenditure per study participant in Germany, one of the world’s wealthiest countries, is more than 33 times the mean expenditure in Tanzania, even when expressed in PPP-adjusted international dollars. That said, with the exception of Germany where 13.1% of the total health expenditure is on mental health, all countries spend 4% or less on these services. These expenditures are low relative to the burden of mental disorders.
Caution must be exercised in making comparisons on the balance of expenditure on care across these countries. Although at first glance Germany and Uganda have similar high proportions of expenditure on inpatient care in our study sample, the relative balance in expenditure on other services was very different. There is an almost complete reliance on inpatient services in Uganda (Kigozi et al., ), with the highest mean number of inpatient stay nights of the five countries. While this analysis does not look specifically at the quality of inpatient care, other studies have previously raised fundamental issues about the protection of human rights and quality of inpatient care in Uganda (Molodynski et al., ). While more recent evaluation suggests the situation in Uganda is improving (Atewologun et al., ), it is critical to further assess the quality of inpatient care. Studies note the absence of mental health services in community settings, although there have been initiatives in rural areas, as part of the national mental health policy framework, to improve access to mental health services in communities by training nurses and primary care workers. However, even this reform did not allow nurses to provide consultations or prescribe medications; this was reported as a barrier to identification and timely treatment at clinics (Kigozi et al., ). While there has been continued development of mental health within primary healthcare services in India (Gajera et al., ), this does not appear to the case in Tanzania, where access to such care nationwide remains very limited (Anonymous, ).
Looking at differences in expenditure by participant characteristics, in contrast to previous international studies (Christensen et al., ; König et al., ; Ride et al., ), we found no associations between healthcare costs and psychiatric diagnoses in any country except India. Similarly, the severity of functional impairment due to mental disorders was not associated with healthcare costs across all countries. Our findings are consistent with the results of a study in the UK (Twomey et al., ) using the HoNOS as a measure for social disability. In contrast, results from other countries indicate clear positive associations between costs and social disability (Eagar et al., ; König et al., ).
One unexpected result of our study was the high cost for outpatient medications in Uganda, which could not be explained simply by the use of UK drug tariffs. However, this result corresponds with an earlier study revealing exceptionally high rates of prescription of second-generation antipsychotics in mental healthcare facilities in Uganda (Rukat, ; Rukat et al., ). Furthermore, we learned from local study workers that the majority of mental health service users commonly received medications at the hospital pharmacy for free, after they were discharged from inpatient care. Unfortunately, we had no further information about the maintenance of drug use after medications received from hospital were used up. More generally, out-of-pocket payments for healthcare are a major barrier to service use in many low- and middle-income countries (Kazibwe et al., ).
Another interesting finding was the low HoNOS (better) score in the Ugandan sample, significantly below the value expected in people with severe mental illness (Mirza et al., ). These lower HoNOS values in the Uganda sample correspond with those from studies assessing the HoNOS at hospital discharge (Jansen et al., ; Luo et al., ), indicating a four-point reduction in HoNOS scores between hospital admission and discharge. This might perhaps be an indicator of improvements in the quality of care, but this needs to be assessed.
Even in high-income countries, there remain stark differences in the balance of services between inpatient care and community-based care. As Table 1 indicates, Germany has a very high rate of psychiatric beds, one of the highest in Europe, helping explain why expenditure is concentrated in psychiatric hospitals. Historically, the structure of the German healthcare system has put much less emphasis on primary care; the shift towards more community-based services is happening more gradually (Mueller-Stierlin et al., ).
Israel has a much more balanced care system, relying more on primary and community care services; nonetheless, it still has extensive access to inpatient beds. Other studies also confirm Israel has a more well-balanced care system with less than 20% of expenditure on inpatient care and a very high proportion of community-based care (Roe et al., ). Community services include many mobile treatments and services to support recovery: mobile multi-disciplinary (occupational therapist, social workers, psychologist, professional team director, etc.) mental health teams, specialist community team/support, vocational rehabilitation, sheltered workshops, vocational support centres and supported employment services (Gal et al., ; Roe et al., ). This more balanced care system is likely to have arisen in part from the implementation of an extensive mental health reform programme that was specifically focused on shifting care out of hospitals.
Strengths and limitations
Our study is the first to investigate costs and factors associated with mental healthcare costs for people with severe mental illness in high-, middle- and low-income countries using individual patient-level data. This allows direct comparisons, for the first time, to be made on associations between service costs and social disability/diagnosis across the five countries.
Limitations result from small country-specific sample sizes and different approaches to study participants’ recruitment in each country. This makes it impossible to assess how representative service user samples are to the population of people with severe mental illness in study countries. The fit parameters of the country-specific GLM reveal differences depending on the different sample sizes. However, the overall model, including data from all countries, seems to fit the data best.
Furthermore, the results regarding the setting-specific distribution of costs must be considered with caution, because they might be biased by national selection procedures. We had to rely on the British National Health Service Drug Tariff for medication unit costs; this actually may be conservative, as the cost of generic medications varies considerably, relative to income in low- and lower-middle-income countries (Liu et al., ). Moreover, these costs are typically funded out of pocket in low- and middle-income countries. A recent review of South Asian countries, including India, highlighted the risk of catastrophic healthcare costs associated with medications for many mental disorders (McDaid et al., ). We also did not look at physical healthcare outcomes and expenditure, despite increased risk of co-morbidity (Hochman et al., ; Liu et al., ). Going forward, there is also scope, using the approach we have adopted, to make further comparisons between greater numbers of countries with different levels of World Bank income classification.
Conclusions
Further research is needed to investigate the associations between the costs of mental healthcare, the balance between in- and outpatient treatment and the quality of mental healthcare in an international comparison. Differences in structure between inpatient treatment and community-based mental healthcare can be explored in future analyses to determine how they impact costs in relation to country-specific levels of economic development. There is also an opportunity to look at the management of mild and moderate mental disorders as services further develop. It would be of particular interest to assess the benefits of improved balance of care to mitigate against low levels of resources in low- and low-middle-income settings.
Acknowledgements
The UPSIDES study is a multicentre collaboration among the Department for Psychiatry and Psychotherapy II at Ulm University, Germany (Bernd Puschner, coordinator); the Institute of Mental Health at University of Nottingham, UK (M.S.); the Department of Psychiatry at University Hospital Hamburg-Eppendorf, Germany (C.M.); Butabika National Referral Hospital, Uganda (J.N.); the Centre for Global Mental Health at London School of Hygiene and Tropical Medicine, UK (G.R.); Ifakara Health Institute, Dar es Salaam, Tanzania (D.S.); the Department of Social Work at Ben Gurion University of the Negev, Be’er Sheva, Israel (G.M.); and the Centre for Mental Health Law and Policy, Pune, India (J.K.).
References
- Addo R, Agyemang SA, Tozan Y and Nonvignon J (2018) Economic burden of caregiving for persons with severe mental illness in sub-Saharan Africa: A systematic review. PLoS One 13, e0199830.
- Anonymous (2021) Mental health in Tanzania deserves some attention. The Citizen, Dar es Saalam.
- Arias D, Saxena S and Verguet S (2022) Quantifying the global burden of mental disorders and their economic value. EClinicalMedicine 54, 101675.
- Atewologun F, Adigun OA, Okesanya OJ, Hassan HK, Olabode ON, Micheal AS, Ahmed MM, Ukoaka BM, Idris NB, Oso TA and Lucero-Prisno DE 3rd (2025) A comprehensive review of mental health services across selected countries in sub-Saharan Africa: Assessing progress, challenges, and future direction. Discover Mental Health 5, 49.
- Charles A, Korde P, Newby C, Grayzman A, Hiltensperger R, Mahlke C, Moran G, Nakku J, Niwemuhwezi J, Nixdorf R, Paul E, Puschner B, Ramesh M, Ryan G, Shamba D, Kalha J and Slade M (2022) Proportionate translation of study materials and measures in a multinational global health trial: Methodology development and implementation. BMJ Open 12, e058083.
- Chisholm D, Knapp MR, Knudsen HC, Amaddeo F, Gaite L, and Van Wijngaarden B (2000) Client Socio-Demographic and Service Receipt Inventory–European Version: Development of an instrument for international research. EPSILON Study 5. European Psychiatric Services: Inputs linked to outcome domains and needs. British Journal of Psychiatry Supplement 39, s28–33.
- Christensen MK, Lim CCW, Saha S, Plana-Ripoll O, Cannon D, Presley F, Weye N, Momen NC, Whiteford HA, Iburg KM and Mcgrath JJ (2020) The cost of mental disorders: A systematic review. Epidemiology and Psychiatric Sciences 29, e161.
- Eagar K, Gaines P, Burgess P, Green J, Bower A, Buckingham B and Mellsop G (2004) Developing a New Zealand casemix classification for mental health services. World Psychiatry 3, 172–177.
- Gajera GV, Pandey P, Malathesh BC, Nirisha PL, Suchandra KHH, Ibrahim FA, Suhas S, Manjunatha N, Kumar CN, Suresha BM and Jain S (2023) Effectiveness of blended versus fully digital training in primary care psychiatry: A retrospective comparison from India. Journal of Neurosciences in Rural Practice 14, 91–97.
- Gal G, Shadmi E, Hoter-Ishay G, Gelkopf M and Roe D (2021) Comparing outcome measures of persons with severe mental illness in vocational rehabilitation programs: A dual perspective of consumers and providers. International Journal for Quality in Health Care 34, ii105–ii111.
- GBD 2019 Mental Disorders Collaborators (2022) Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. The Lancet Psychiatry 9, 137–150.
- Hochman L, Moran GS, Gelkopf M, Roe D and Shadmi E (2021) Prospectively identifying adults with serious mental illness at risk for poor physical health: The role of person reported outcomes. International Journal for Quality in Health Care 34, ii65–ii69.
- Husereau D, Drummond M, Augustovski F, De Bekker-Grob E, Briggs AH, Carswell C, Caulley L, Chaiyakunapruk N, Greenberg D, Loder E, Mauskopf J, Mullins CD, Petrou S, Pwu RF and Staniszewska S (2022) Consolidated Health Economic Evaluation Reporting Standards 2022 (CHEERS 2022) statement: Updated reporting guidance for health economic evaluations. Value in Health 25, 3–9.
- International Monetary Fund. 2022. Implied PPP conversion rate [Online]. https://www.imf.org/external/datamapper/PPPEX@WEO/OEMDC/ADVEC/WEOWORLD (accessed 10 June 2025).
- Jaeschke K, Hanna F, Ali S, Chowdhary N, Dua T and Charlson F (2021) Global estimates of service coverage for severe mental disorders: Findings from the WHO Mental Health Atlas 2017. Global Mental Health 8, e27.
- Jansen L, Hunnik F, Busschbach JJV and Lijmer JG (2019) Measuring outcomes on a Medical Psychiatric Unit: HoNOS, CANSAS and costs. Psychiatry Research 280, 112526.
- Kazibwe J, Tran PB and Annerstedt KS (2021) The household financial burden of non-communicable diseases in low- and middle-income countries: A systematic review. Health Research Policy and Systems 19, 96.
- Kigozi FN, Kizza D, Nakku J, Ssebunnya J, Ndyanabangi S, Nakiganda B, Lund C and Patel V (2016) Development of a district mental healthcare plan in Uganda. British Journal of Psychiatry 208(Suppl 56), s40–6.
- Kilian R, Matschinger H, Löeffler W, Roick C and Angermeyer MC (2002) A comparison of methods to handle skew distributed cost variables in the analysis of the resource consumption in schizophrenia treatment. Journal of Mental Health Policy and Economics 5, 21–31.
- Knapp M and Beecham J (1990) Costing mental health services. Psychological Medicine 20, 893–908.
- König H, König HH, Gallinat J, Lambert M, Karow A, Peth J, Schulz H and Konnopka A (2022) Excess costs of mental disorders by level of severity. Social Psychiatry & Psychiatric Epidemiology 58, 973–985.
- Liu NH, Daumit GL, Dua T, Aquila R, Charlson F, Cuijpers P, Druss B, Dudek K, Freeman M, Fujii C, Gaebel W, Hegerl U, Levav I, Munk Laursen T, Ma H, Maj M, Elena Medina‐Mora M, Nordentoft M, Prabhakaran D, Pratt K, Prince M, Rangaswamy T, Shiers D, Susser E, Thornicroft G, Wahlbeck K, Fekadu Wassie A, Whiteford H and Saxena S (2017) Excess mortality in persons with severe mental disorders: A multilevel intervention framework and priorities for clinical practice, policy and research agendas. World Psychiatry 16, 30–40.
- Luo W, Harvey R, Tran T, Phung D, Venkatesh S and Connor JP (2016) Consistency of the Health of the Nation Outcome Scales (HoNOS) at inpatient-to-community transition. BMJ Open 6, e010732.
- Mahapatra P and Seshadri S (2024) Mental health in India: Evolving strategies, initiatives, and prospects. The Lancet Regional Health – Southeast Asia 20, 100300.
- McCullagh P, and Nelder J A (1989) Generalized Linear Models 2. Boca Raton: Chapman & Hall / CRC 532.
- McDaid D, Vidyasagaran AL, Nasir M, Walker S, Wright J, Muliyala KP, Thekkumkara S, Huque R, Faisal MR, Benkalkar S, Kabir MA, Russell C, and Siddiqi N (2024) Understanding the costs and economic impact of mental disorders in South Asia: A systematic review. Asian Journal of Psychiatry 102, 104239.
- Metreau E, Young KE and Eapen SG 2024. World Bank country classifications by income level for 2024-2025. https://blogs.worldbank.org/en/opendata/world-bank-country-classifications-by-income-level-for-2024-2025 (accessed ).
- Mirza L, Das-Munshi J, Chaturvedi J, Wu H, Kraljevic Z, Searle T, Shaari S, Mascio A, Skiada N, Roberts A, Bean D, Stewart R, Dobson R and Bendayan R (2021) Investigating the association between physical health comorbidities and disability in individuals with severe mental illness. European Psychiatry 64, e77.
- Mokgobi MG (2014) Understanding traditional African healing. African Journal for Physical Health Education, Recreation and Dance 20, 24–34.
- Molodynski A, Cusack C and Nixon J (2017) Mental healthcare in Uganda: Desperate challenges but real opportunities. BJPsych International 14, 98–100.
- Moran GS, Kalha J, Mueller-Stierlin AS, Kilian R, Krumm S, Slade M, Charles A, Mahlke C, Nixdorf R, Basangwa D, Nakku J, Mpango R, Ryan G, Shamba D, Ramesh M, Ngakongwa F, Grayzman A, Pathare S, Mayer B and Puschner B (2020) Peer support for people with severe mental illness versus usual care in high-, middle- and low-income countries: Study protocol for a pragmatic, multicentre, randomised controlled trial (UPSIDES-RCT). Trials 21, 371.
- Mueller-Stierlin AS, Dinc U, Herder K, Walendzik J, Schuetzwohl M, Becker T and Kilian R (2022) The cost-effectiveness analysis of an integrated mental health care programme in Germany. International Journal of Environmental Research & Public Health 19, 6814.
- National Health Service Business Service Authority (NHSBSA) (2022) NHS drug tariff [Online]. https://www.nhsbsa.nhs.uk/pharmacies-gp-practices-and-appliance-contractors/drug-tariff (accessed August ).
- OECD (2021) A New Benchmark for Mental Health Systems: Tackling the Social and Economic Costs of Mental Ill-health. Paris: OECD Publishing.
- Omigbodun OO, Ryan GK, Fasoranti B, Chibanda D, Esliker R, Sefasi A, Kakuma R, Shakespeare T and Eaton J (2023) Reprioritising global mental health: Psychoses in sub-Saharan Africa. International Journal of Mental Health Systems 17, 6.
- Patel V, Saxena S, Lund C, Thornicroft G, Baingana F, Bolton P, Chisholm D, Collins PY, Cooper JL, Eaton J, Herrman H, Herzallah MM, Huang Y, Jordans MJD, Kleinman A, Medina-Mora ME, Morgan E, Niaz U, Omigbodun O, Prince M, Rahman A, Saraceno B, Sarkar BK, De Silva M, Singh I, Stein DJ, Sunkel C and Unützer J (2018) The Lancet Commission on global mental health and sustainable development. The Lancet 392, 1553–1598.
- Rajkumar RP (2022) The correlates of government expenditure on mental health services: An analysis of data from 78 countries and regions. Cureus 14, e28284.
- Ride J, Kasteridis P, Gutacker N, Aragon Aragon MJ and Jacobs R (2020) Healthcare costs for people with serious mental illness in England: An analysis of costs across primary care, hospital care, and specialist mental healthcare. Applied Health Economics and Health Policy 18, 177–188.
- Roe D, Mashiach-Eizenberg M, Garber Epstein P, Yamin A, Hoter Ishay G and Zisman-Ilani Y (2021) Implementation of NAVIGATE for first episode psychosis in Israel: Clients’ characteristics, program utilization and ratings of change. Early Intervention in Psychiatry 15, 1343–1348.
- Rukat A (2015) Diagnostische Praxis und Verschreibungsmuster in Psychiatrischen Kliniken in Uganda. Dissertation, Berlin, pp. 6–11.
- Rukat A, Musisi S, Ströhle A and Mundt AP (2014) Prescription patterns of psychotropic medications for the treatment of psychotic disorders in the largest mental health institutions of Uganda. Journal of Clinical Psychopharmacology 34, 571–576.
- Slade M, Powell R, Rosen A, and Strathdee G (2000) Threshold Assessment Grid (TAG): The development of a valid and brief scale to assess the severity of mental illness. Social Psychiatry & Psychiatric Epidemiology 35, 78–85.
- StataCorp (2021) Stata Statistical Software: Release 17. College Station, TX.
- Thornicroft G and Tansella M (2013) The balanced care model for global mental health. Psychological Medicine 43, 849–863.
- Twomey C, Prina AM, Baldwin DS, Das-Munshi J, Kingdon D, Koeser L, Prince MJ, Stewart R, Tulloch AD and Cieza A (2016) Utility of the Health of the Nation Outcome Scales (HoNOS) in predicting mental health service costs for patients with common mental health problems: Historical cohort study. PLoS One 11, e0167103.
- Wiegand HF, Lars H, Oliver T, Klaus L, Peter F and Adorjan K (2025) Mental health services in Germany – Structures, outcomes and future challenges. International Review of Psychiatry 1–18.
- Wing JK, Beevor AS, Curtis RH, Park SB, Hadden S and Burns A (1998) Health of the Nation Outcome Scales (HoNOS). Research and development. British Journal of Psychiatry 172, 11–18.
- Wing J, Lelliott P and Beevor A (2000) Progress on HoNOS. The British Journal of Psychiatry 176, 392–393.
- World Bank (2020) World Bank Country and Lending Groups. Washington D.C.: World Bank.
- World Health Organization (2021a) Comprehensive Mental Health Action Plan 2013–2030. Geneva: World Health Organization.
- World Health Organization (2021b) Mental Health Atlas 2020. Geneva: World Health Organization.