Introduction
Cochlear implantation (CI) is nowadays considered a safe and efficient procedure to rehabilitate severe to profound sensorineural hearing loss, both in adults and in children. The standardized guidelines for rehabilitating an adult with a CI are (1) severe to profound bilateral sensorineural hearing loss, with little or insufficient benefit from conventional hearing aids and (2) a speech discrimination score lower than 50%. When the hearing loss is bilateral, different strategies are available for the restoration of the binaural hearing, including bilateral CIs or a combination of a CI and a hearing aid (HA) in the contralateral ear. The benefits of binaural hearing are well described in the literature - and can be summarized to (1) a binaural redundancy and summation effect, allowing a better discrimination of phonemes, words, and phrases, either in quiet or in noisy ambient conditions and (2) a better localization of incoming sound stimuli due to the head shadow effect. The aim of this article is to describe the different rehabilitation audiological patterns of 71 adult patients, affected by severe to profound sensorineural hearing loss, aided by CIs and HAs.
Patients and Methods
This is a retrospective study assessing information from past clinical records. Data from adult patients presenting severe to profound sensorineural hearing loss who received a CI, between February 2011 and December 2018, at the Audiology department of our University Hospital, were considered.
The various cases were assigned to the study after satisfying the following criteria: (1) patient’s age >20 years and (2) the case was related to a single or a double CI surgery. A total of 71 cases (30 females and 41 males) were considered suitable for the analysis, and the data assessed from the corresponding clinical records included the following:
The age at the time of the surgery: According to the patient’s age at the time of the surgery, patients were assigned in 3 age groups, such as group A: 20 to 39 years; group B: 40 to 64 years; and group C >65 years;
the hearing loss etiology (if available);
the date of the first/second CI surgery;
the use of hearing aids prior to the CI;
the auditory threshold (pure tone average at 500-1000-2000-4000 Hz) at pre and at 6 months postoperation; and
Data from the speech recognition tests: A speech audiometry (without background noise at 60 dB) was performed in order to evaluate speech recognition at 6 months postsurgery. Additional speech tests, using the disyllabic words repetition test and the phonetic matrices test were conducted at 12 months postsurgery. Binaural hearing in speech audiometry (without background noise competition at 60 dB) was also tested, using the disyllabic words repetition test and the phonetic matrices test.
The research protocol was conducted in compliance with the Helsinki Declaration (2008); the study was observational; it was performed retrospectively through a case record review and therefore did not affect patient care in any way. However, all patients were informed about the project during their consequent visits and provided their participation consent.
Statistical Analysis
The data were analysed using SPSS version 23 for windows. The t test and analysis of variance procedures were used to evaluate quantitative normal parameters. Statistical significance was considered at P < .05.
Results
The patients were assigned to 3 age groups, with the following characteristics:
Group A (20-39 years) included 20 (28%) patients: Four patients with a unilateral CI, 9 patients with a sequential bilateral CI, and 7 patients with unilateral CI and a hearing aid at the contralateral ear.
Group B (40-64 years) included 25 (35%) patients: Four patients with a unilateral CI, 7 patients with a sequential bilateral CI, and 14 patients with unilateral CI and hearing aid at the contralateral ear.
Group C (>65 years) included 26 (37%) patients: Eight patients with a unilateral CI, 5 patients with a sequential bilateral CI, and 13 patients with unilateral CI and a hearing aid at the contralateral ear.
Concerning the onset of hearing loss, 10 (14%) patients had prelingual hearing loss, 2 (3%) patients had perilingual hearing loss, and 59 (83%) patients had postlingual hearing loss.
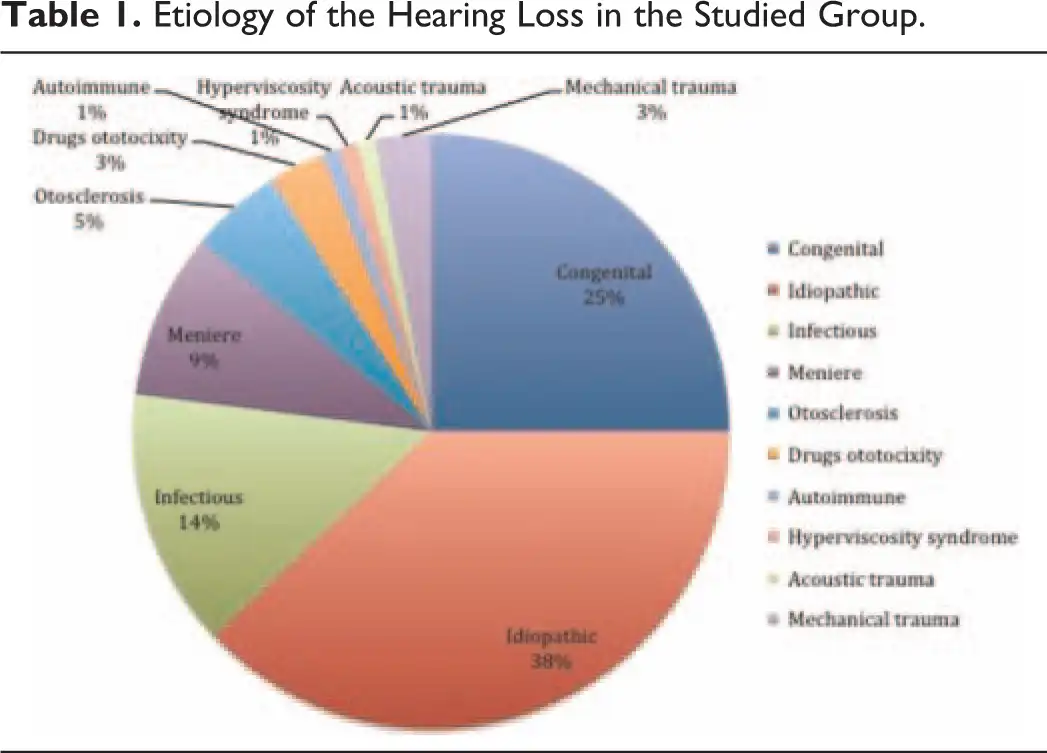
The etiology of hearing loss was identified only in 62% of cases (see Table 1) and the main causes were infections (14%), such as meningitis or chronic recurrent otitis media; otosclerosis (5%); Ménière disease (9%); ototoxic drugs (3%); acoustic trauma (1%); autoimmune diseases (1%); and congenital forms (25%). Among the latter, the etiology remained unknown for 4 cases; inner ear malformation was identified in 1 case; nonsyndromic deafness was identified in 7 cases; and syndromic deafness was identified in 5 patients. The identified genetic diseases were the Kearns-Sayre syndrome, the Usher syndrome, the Cogan syndrome, and the Marfan syndrome (see Table 1).
According to the rehabilitative choice for the contralateral ear, the patients were divided into 3 groups:
group 1: 16 (22.5%) patients with a unilateral CI;
group 2: 21 (29.5%) patients with a bilateral CI; and
group 3: 34 (47%) patients with a unilateral CI and a hearing aid in the contralateral ear (bimodal stimulation).
All patients underwent tonal audiometry testing before and after CI; The postimplantation pure tone average (PTA) values did not show any statistically significant differences, considering the rehabilitative choice of the contralateral ear and the age-group.
Data on binaural hearing were available for only 55 patients: 21 with a bilateral CI and 34 with bimodal hearing. In particular, at 6 months from the CI surgery, all 55 patients were assessed by a speech recognition vocal test at 60 dB in a soundproof cabin obtaining a mean value of 78.9% ± 19.8% (no significant differences were observed considering the rehabilitative choice of the contralateral ear and the age-group). At 12 months postsurgery, speech recognition was tested by repeating bisyllabic words and phonetic matrices (vowel, consonant, vowel), obtaining a mean value of 82.6% ± 16.8 and 77.5% ±14.3%, respectively, with the age group C (40-60 years) having the worst performance, especially with bisyllabic words.
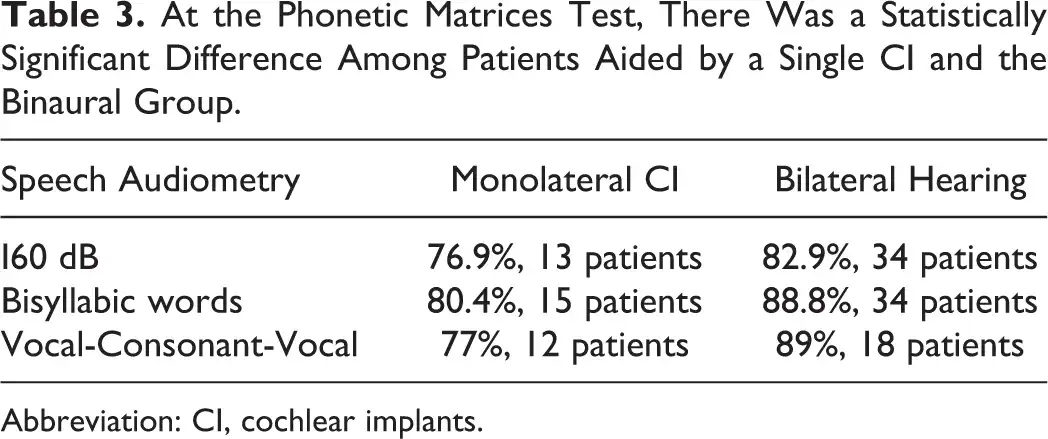
The unilateral CI group data were compared to the data from the binaural group (bilateral CI OR CI + hearing aid) by testing speech recognition with a vocal test at 60 dB and by repeating bisyllabic words and phonetic matrices (vowel, consonant, vowel; see Tables 2 and 3). At the vocal test, there were no statistically significant differences among the groups. By repeating bisyllabic words and phonetic matrices, statistically significant differences were observed between the unilateral CI patients (81.3% ± 18%) and the patients from the binaural group (bilateral CIs = 87.3% ± 14%; CI + HA = 81.1% ±15%).

Discussion
Nowadays, hearing rehabilitation of severe to profound sensorineural hearing loss includes the selection of CIs and/or eventually of hearing aids, with the aim of resolving the communication problems of the affected individuals. , Patients affected by severe to profound sensorineural hearing impairment usually have a significant loss or dysfunction of their inner ears (hair cells and/or spiral ganglion neurons). In fact, when fitting hearing aids, the range from threshold to uncomfortable loudness is often very small for these individuals and with possible variations at each frequency. For these reasons, the use of HA for the rehabilitation of these patients is often limited as well as the information that can be transferred through the auditory pathway by these devices. , On the other hand, nowadays, CIs represent a safe and efficient procedure for those affected by severe to profound hearing loss. By directly stimulating the spiral ganglion nerves fibres, these devices can properly activate the auditory pathway, offering an overall worth hearing performance. ,
If possible, a bilateral stimulation should be always preferred. Binaural hearing should be restored by using a bilateral CI or a CI and hearing aid in the contralateral ear (bimodal stimulation). Benefits of binaural hearing mainly include (1) binaural redundancy and summation effects that allow a better discrimination of speech including phonemes, words, and phrases, either in quiet or in noisy situations and (2) localization of sounds due to head shadow effect. However, binaural hearing also improves listening in noise and influences a more positive satisfaction of hearing-impaired patients. It has also been reported that it can improve cognitive tasks such as short-term memory as well as reducing social isolation and symptoms of depression. -
The data from our study show the beneficial effects of binaural hearing, and in particular at the phonetic matrices test, as the binaural group performed statistically significantly better than those aided by a single CI. A major drawback of this study is the absence of data on spatial hearing of the studied group, which were not collected in the past.
According to data in the literature, binaural hearing (CI and hearing aid in the contralateral ear) offers better results at the speech audiometry tests, at least 6 months after surgery, - than a single CI. In particular, bilateral CIs have been reported to offer a better hearing performance and an improved subjective quality-of-life perception than bimodal hearing (CI and hearing aid in the contralateral ear). Also, according to Yawn et al, bilateral CI patients perform significantly better when testing consonant-nucleus-consonant speech recognition than their pairs aided by a bimodal hearing. Also, Granço et al reported a greater satisfaction level for bilateral CIs adult users examining their levels of speech perception.
Some considerations should be taken among the duration of hearing deprivation, and/or the period of inadequate stimulation, as these are reported to negatively influence the outcome of hearing rehabilitation by several authors, as expected. - In fact, for adults affected by severe to profound sensorineural hearing loss, it is often difficult to investigate and to estimate with precision the length of hearing deprivation or of improper hearing stimulation. - Unfortunately, we could not retrieve these information in the present studied group.
For most adults with severe to profound sensorineural hearing loss, especially if hearing loss is acquired progressively, the loss of conversational fluency represents a major problem. ,, - These patients, on the one hand, should be rehabilitated, bilaterally, by proper devices (CI and HA or bilateral CI). In some cases, they should also be helped to set strategies (such as such as maintaining eye contact and asking to face the speaker; speaking more slowly and eventually rephrasing) in order to experience an overall good hearing level in different auditory scenes. ,, -
In conclusion, according to the present data, binaural hearing (either with a bilateral CI or bimodal) allows an improvement in the functional results at the speech tests compared to the use of a CI only.
Acknowledgments
The authors wish to thank Prof Claudia Aimoni for her support in preparing the manuscript.
Declaration of Conflicting Interests The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- 1. Marsella P, Giannantonio S, Scorpecci A, Pianesi F, Micardi M, Resca A. Role of bimodal stimulation for auditory-perceptual skills development in children with a unilateral cochlear implant. Acta Otorhinolaryngol Ital. 2015;35(6):442–448.
- 2. Litovsky RY, Johnstone PM, Godar SP. Benefits of bilateral cochlear implants and/or hearing aids in children. Int J Audiol. 2006;45(1):S78–S91.
- 3. Litovsky RY, Johnstone PM, Godar S, et al. Bilateral cochlear implants in children: localization acuity measured with minimum audible angle. Ear Hear. 2006;27(1):43–59.
- 4. Ching TY, van Wanrooy E, Hill M, Incerti P. Performance in children with hearing aids or cochlear implants: bilateral stimulation and binaural hearing. Int J Audiol. 2006;45(1):S108–112.
- 5. Litovsky RY, Parkinson A, Arcaroli J. Spatial hearing and speech intelligibility in bilateral cochlear implant users. Ear Hear. 2009;30(4):419–431.
- 6. Skinner MW, Binzer SM, Potts LG, Holden LK, Aaron RJ. Hearing rehabilitation for individuals with severe and profound hearing impairment: hearing aids, cochlear implants and counselling. In Valente M, ed. Strategies for Selecting and Verifying Hearing Aids Fittings. New York, NY: Thieme; 2002:311–344.
- 7. Turunen-Taheri S, Carlsson PI, Johnson AC, Hellström S. Severe-to-profound hearing impairment: demographic data, gender differences and benefits of audiological rehabilitation. Disabil Rehabil. 2019;41(23):2766–2774.
- 8. Guo S, Li H, Chen B, Dai C. Study of categories of auditory performance and speech intelligibility rating of post-lingualcochlear implantes. Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2014;28(13):955–957.
- 9. Granço FS, Fernandes NF, Morettin M, Filho OA, Bevilacqua MC. The relationship between the speech perception and the degree of satisfaction among adult users of cochlear implants. Int Arch Otorhinolaryngol. 2013;17(2):202–207.
- 10. Yawn RJ, O’Connell BP, Dwyer RT, et al. Bilateral cochlear implantation versus bimodal hearing in patients with functional residual hearing: a within-subjects comparison of audiologic performance and quality of life. Otol Neurotol. 2018;39(4):422–427.
- 11. Garcia-Iza L, Martinez Z, Ugarte A, Fernandez M, Altuna X. Cochlear implantation in the elderly: outcomes, long-term evolution, and predictive factors. Eur Arch Otorhinolaryngol. 2018;275(4):913–922.
- 12. Pimperton H, Walker EA. Word learning in children with cochlear implants: examining performance relative to hearing peers and relations with age at implantation. Ear Hear. 2018;39(5):980–991.
- 13. Eapen RJ, Buss E, Adunka MC, Pillsbury HC III, Buchman CA. Hearing in noise benefits after bilateral simultaneous cochlear implantation continue to improve 4 years after implantation. Otol Neurotol. 2009;30(2):153–159.
- 14. Wackym PA, Runge-Samuelson CL, Firszt JB, Alkaf FM, Burg LS. More challenging speech-perception tasks demonstrate binaural benefit in bilateral cochlear implant users. Ear Hear. 2007;28(2):80S–85S.
- 15. Litovsky R, Parkinson A, Arcaroli J, Sammeth C. Simultaneous bilateral cochlear implantation in adults: a multicenter clinical study. Ear Hear. 2006;27(6):714–731.
- 16. Ramsden R, Greenham P, O’Driscoll M, et al. Evaluation of bilaterally implanted adult subjects with the nucleus 24 cochlear implant system. Otol Neurotol. 2005;26(5):988–998.
- 17. Berrettini S., Baggiani A, Bruschini L, et al. Systematic review of the literature on the clinical effectiveness of the cochlear implant procedure in adult patients. Acta Otorhinolaryngol Ital. 2011;31(5):299–310.
- 18. Derinsu U, Yüksel M, Geçici CR, Çiprut A, Akdeniz E. Effects of residual speech and auditory deprivation on speech perception of adult cochlear implant recipients. Auris Nasus Larynx. 2019;46(1):58–63.
- 19. Medina MDM, Polo R, Gutierrez A, et al. cochlear implantation in postlingual adult patients with long-term auditory deprivation. Otol Neurotol. 2017;38(8):e248–e252.
- 20. Beyea JA, McMullen KP, Harris MS, et al. Cochlear implants in adults: effects of age and duration of deafness on speech recognition. Otol Neurotol. 2016;37(9):1238–1245.
- 21. Kong YY, Carlyon RP. Improved speech recognition in noise in simulated binaurally combined acoustic and electric stimulation. J Acoust Soc Am. 2007;121(6):3717–3727.
- 22. Vermeire K, Van de Heyning P. Binaural hearing after cochlear implantation in subjects with unilateral sensorineural deafness and tinnitus. Audiol Neurootol. 2008;14(3):163–171.
- 23. Litovsky RY, Goupell MJ, Godar S, et al. Studies on bilateral cochlear implants at the University of Wisconsin’s Binaural Hearing and Speech Laboratory. J Am Acad Audiol. 2012;23(6):476–494.
- 24. Ching TYC, Incerti P, Hill M. Binaural benefits for adults who use hearing aids and cochlear implants in opposite ears. Ear Hear. 2004;25(1):9–21.
- 25. Cullington HE, Zeng F. Bimodal hearing benefit for speech recognition with competing voice in cochlear implant subject with normal hearing in contralateral ear. Ear Hear. 2010;31(1):70–73.
- 26. Warren SE, Dunbar MN. Bimodal hearing in individuals with severe-to-profound hearing loss: benefits, challenges, and management. Semin Hear. 2018;39(4):405–413.
- 27. Gifford RH, Dorman MF. Bimodal hearing or bilateral cochlear implants? ask the patient. Ear Hear. 2019;40(3):501–516.
- 28. Firszt JB, Reeder RM, Holden LK, Dwyer NY. Asymmetric Hearing Study Team. Results in adult cochlear implant recipients with varied asymmetric hearing: a prospective longitudinal study of speech recognition, localization, and participant report. Ear Hear. 2018;39(5):845–862.
- 29. Sanhueza I, Manrique-Huarte R, Calavia D, Huarte A, Manrique M. Hearing impairment and quality of life in adults with asymmetric hearing loss: benefits of bimodal stimulation. J Int Adv Otol. 2019;15(1):62–69.