Significance Statement: Overmedialization with a laryngeal implant is a possible complication following type I thyroplasty to treat glottic insufficiency. Evaluation of this complication can be performed in ambulatory settings using laryngeal palpation with anterior-posterior manual compression that partially relieves the effects of overmedialization (especially anterior overmedialization) on voice.
A 28-year-old man presented to the office for a second opinion regarding hoarseness that followed intubation for cardiac arrest. He described a weak and raspy voice that had become more strained and effortful over time despite several laryngologic procedures and voice therapy. Prior to presentation to the senior author (RTS), he had undergone a series of vocal fold injection laryngoplasties (most recently, left vocal fold injection with calcium hydroxylapatite), as well as a right type I thyroplasty with a silicone implant. Strobovideolaryngoscopy (SVL) revealed right-worse-than-left vocal fold paresis (confirmed by laryngeal EMG), vocal fold stiffness worse on the left, and excessive fullness at the anterior commissure (Figure 1). This was confirmed with computed omography (CT) of the larynx (Figure 2) showing the implant situated slightly too anteriorly and medially. Calcium hydroxylapatite was visualized on the left side. Anterior-to-posterior compression of the thyroid cartilage in the office decreased the severity of pressed phonation. Surgical removal of the silicone implant improved voice quality and with reduced voice strain. Because calcium hydroxylapatite was still present on the left, it was decided preoperatively that no further permanent adjustments would be made until that material had resorbed. On follow-up 1 month after surgery, the patient reported less effort with phonation, despite sounding somewhat breathier (as was expected). Revision type 1 thyroplasty was performed at a later time.
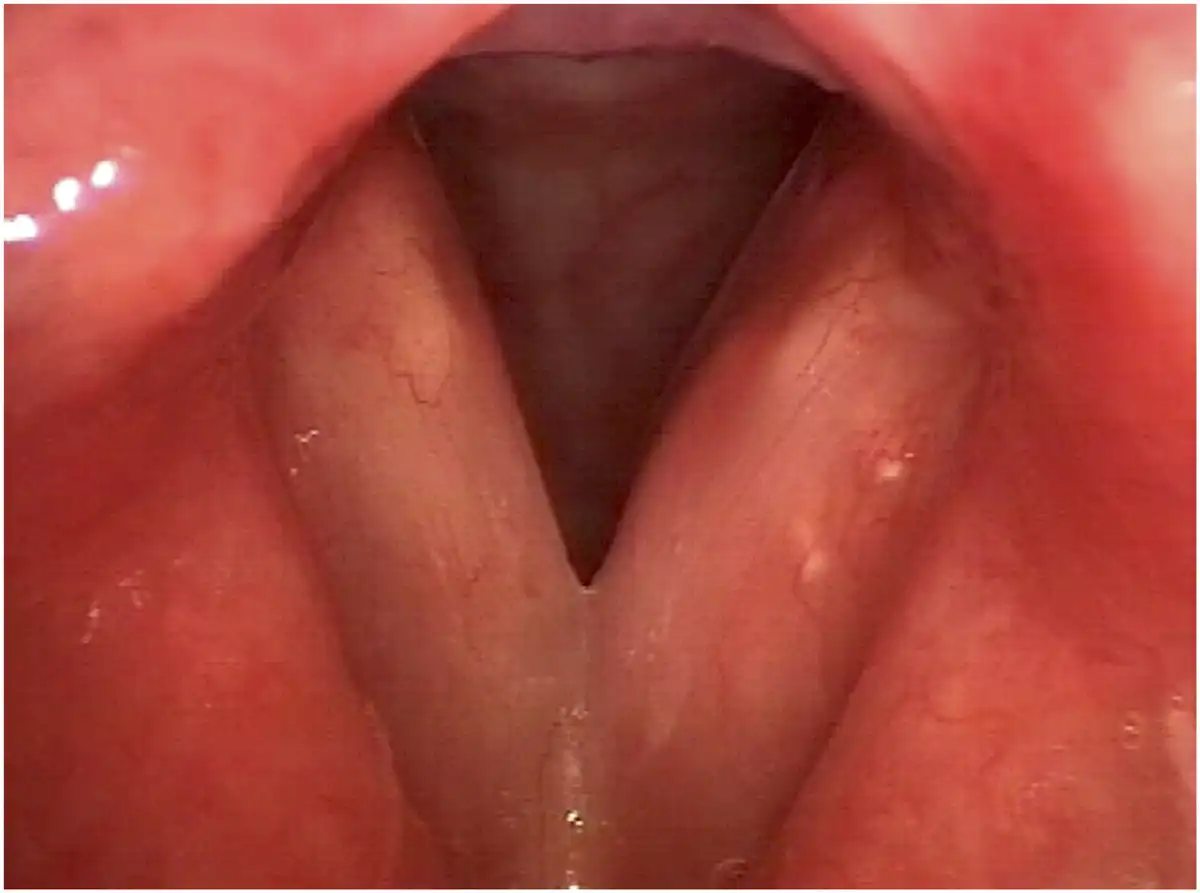
Figure 1
Strobovideolaryngoscopy with 70° rigid endoscope shows fullness at the anterior commissure.
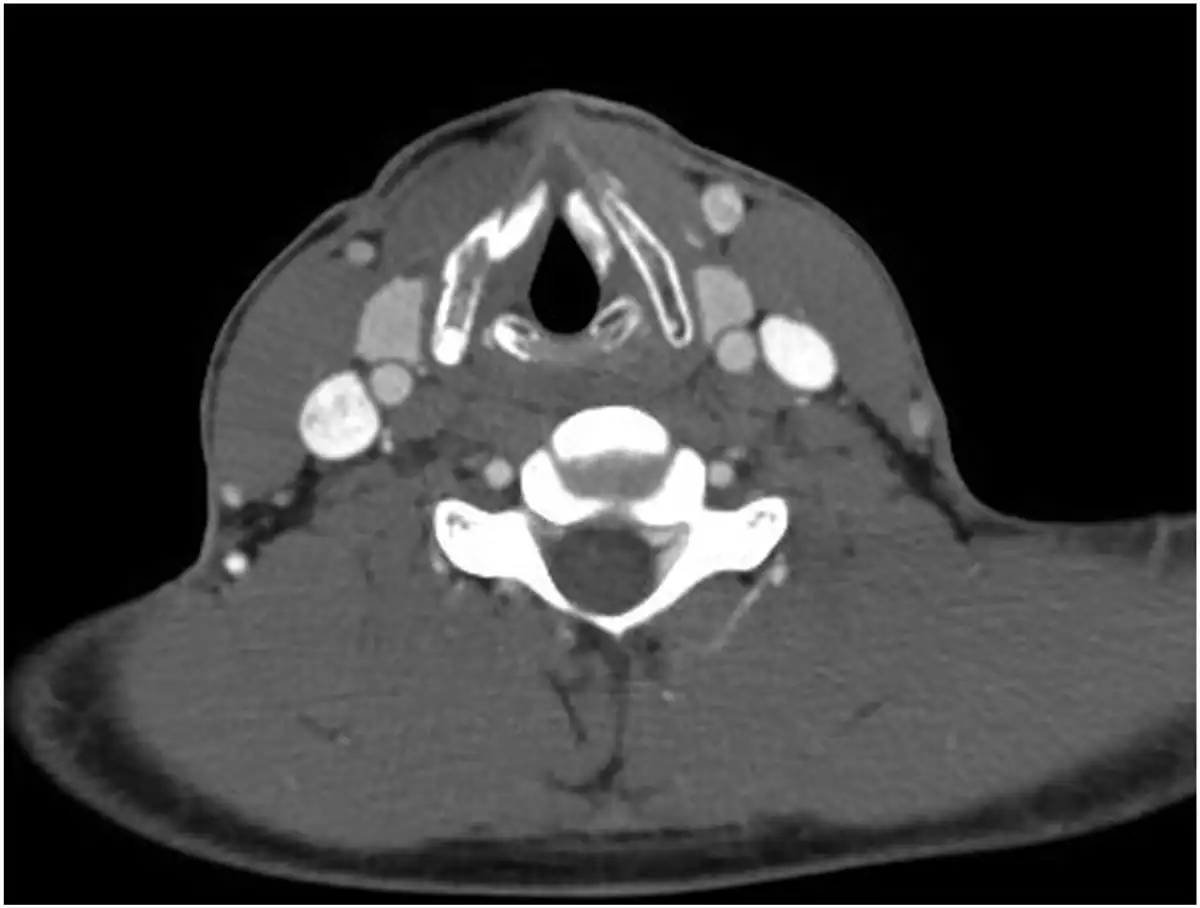
Figure 2
CT of the larynx (axial view) at the level of the true vocal folds shows a Silastic implant that is slightly overmedializing the right vocal fold at the anterior commissure. The calcium hydroxylapatite injected into the left side also can be seen.
Type I thyroplasty is a procedure that treats glottic insufficiency due to a variety of causes. Overmedialization is a potential complication. This often results in a voice that sounds pressed or strained, and the patient may complain of increased effort with phonation. A 1993 review by Wanamaker et al. studied the outcomes of 160 type I thyroplasties with 83 patients having a silicone implant. Of those 83 patients, 9 needed a revision surgery with placement of a larger implant. No cases of revision surgery with placement of a smaller implant were reported. This trend in the literature might be the result of the challenges associated with identification of an implant that is overmedialized as opposed to one that is undermedialized with an obvious persistent glottic gap on SVL.
Manual compression with laryngeal palpation plays a role as a simple and non-invasive maneuver that can be used in the office setting to aid in the diagnosis of overmedialization and undermedialization from laryngeal implants. Manual laryngeal compression is used most often to simulate the effect of medializing the vocal folds; however, anterior-to-posterior compression at the midline of the thyroid cartilage can provide an estimation of the effect of decreasing overmedialization near the anterior commissure such as that which occurred in the case presented. The voice immediately became less strained and pressed. At the time of surgery, this change in voice was observed when the implant had been removed. Presumably, the capsule that had formed around the implant provided some degree of medialization even after the implant was removed. Further studies on the efficacy of this technique as a predictor of overmedialization may be worthwhile.
Author Contributions A.A.S.: Manuscript development. Revision of protocol and manuscript.
Author Contributions K.A.K.: Data collection and analysis. Drafting manuscript.
Author Contributions H.A.Y.: Drafting of protocol and manuscript. Revision of protocol and manuscript. Project supervision.
Author Contributions A.J.J.: Data collection and analysis. Revision of protocol and manuscript. Project supervision.
Author Contributions R.T.S.: Project oversight. Data analysis. Drafting of protocol and manuscript. Revision of protocol and manuscript.
Declaration of Conflicting Interests The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- 1. Wanamaker JR, Netterville JL, Ossoff RH. Silastic medialization for unilateral vocal fold paralysis. Oper Tech Otolaryngol Head Neck Surg. 1993;4(3):207–217.
- 2. Blaugrund SM, Taira T, el-Assuooty A, Lin PT, Isshiki N, Gould WJ. Effects of lateral manual compression upon glottis incompetence: Objective evaluations. Ann Otol Rhinol Laryngol. 1990;99(4 pt 1):249–255.