Corresponding Article
This Month's Highlights
Journal of the American Society of Nephrology 31(8):p i-i, August 2020. | DOI: 10.1681/ASN.2020060907
Although arteriovenous fistulas (AVFs) are the vascular access modality of choice for patients with established renal failure, high early failure rates limit universal use. Brachial plexus block—regional anesthesia—at the time of AVF creation provides sympathetic blockade and produces venodilation; several studies have demonstrated associated improvement in AVF patency rates. The authors demonstrate for the first time that these perioperative changes translate into sustained improvement in functional patency at 1 year after AVF creation under regional anesthesia compared with local anesthesia. Cost-effectiveness analyses showed that this more labor-intensive technique resulted in net savings. These findings suggest that regional anesthesia has potential to improve AVF usage among the dialysis population, avoid complications of alternative access modalities, reduce surgical workload, and deliver cost savings to healthcare systems at large.
Regional anesthesia improves short-term blood flow through arteriovenous fistulas (AVFs). We previously demonstrated that, compared with local anesthesia, regional anesthesia improves primary AVF patency at 3 months.
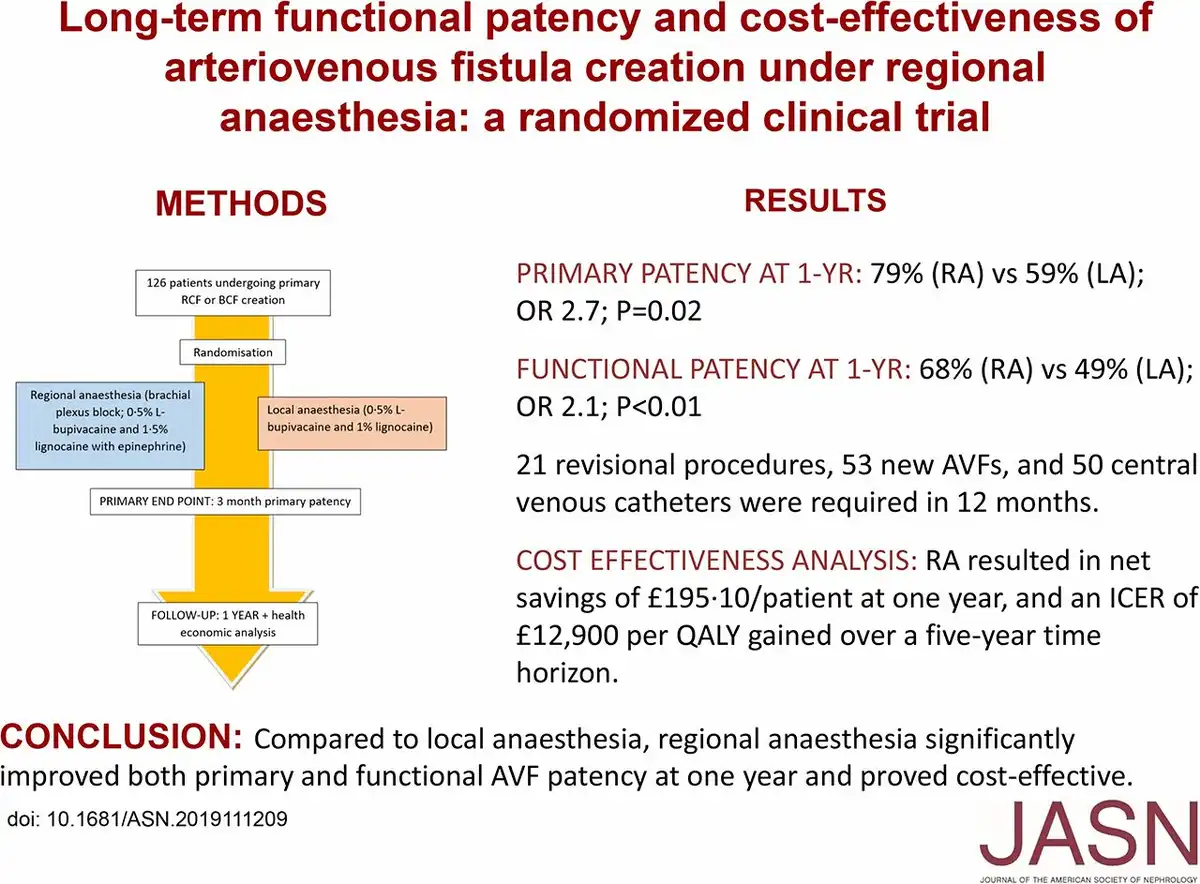
To study the effects of regional versus local anesthesia on longer-term AVF patency, we performed an observer-blinded randomized controlled trial at three university hospitals in Glasgow, United Kingdom. We randomly assigned 126 patients undergoing primary radiocephalic or brachiocephalic AVF creation to receive regional anesthesia (brachial plexus block; 0.5% L-bupivacaine and 1.5% lidocaine with epinephrine) or local anesthesia (0.5% L-bupivacaine and 1% lidocaine). This report includes findings on primary, functional, and secondary patency at 12 months; reinterventions; and additional access procedures (primary outcome measures were previously reported). We analyzed data by intention to treat, and also performed cost-effectiveness analyses.
At 12 months, we found higher primary patency among patients receiving regional versus local anesthesia (50 of 63 [79%] versus 37 of 63 [59%] patients; odds ratio [OR], 2.7; 95% confidence interval [95% CI], 1.6 to 3.8; P=0.02) as well as higher functional patency (43 of 63 [68%] versus 31 of 63 [49%] patients; OR, 2.1; 95% CI, 1.5 to 2.7; P=0.008). In 12 months, 21 revisional procedures, 53 new AVFs, and 50 temporary dialysis catheters were required. Regional anesthesia resulted in net savings of £195.10 (US$237.36) per patient at 1 year, and an incremental cost-effectiveness ratio of approximately £12,900 (US$15,694.20) per quality-adjusted life years over a 5-year time horizon. Results were robust after extensive sensitivity and scenario analyses.
Compared with local anesthesia, regional anesthesia significantly improved both primary and functional AVF patency at 1 year and is cost-effective.
Local Anaesthesia versus Regional Block for Arteriovenous Fistulae, NCT01706354