1 INTRODUCTION
Humans have been exposed to varying levels of visible and invisible light since the beginning of their development on earth. Moreover, the inescapable consequences of industrialization and global modernization have caused enormous changes in people's lifestyles in both developing and developed countries during the past few decades. Humans are now overexposed to artificial light during days and nights and do not receive adequate natural light during the day. Artificial lights have been incorporated into daily life as a result of digitization, which has led to light pollution. To make the days longer for work or for modern life, artificial light has been produced. Therefore, our body no longer gets the cues it previously did to get ready for sleep and act according to normal circadian rhythm. The change in the evening and night time light has also an adverse effect on our body circadian rhythm and general health. The skin, as the biggest organ in the body, is immediately exposed to both artificial and environmental light and the outside trauma. It serves as the initial line of protection against environmental hazards. The skin has also shown to have a substantial circadian rhythm due to its many activities. During the day, these functions are more protected, while at night or during darkness, they are more suited for repair. The effect of light on the skin has also therapeutic indications. Digital screens are among the latest methods of nonthermal light treatment that dermatologists may use. LEDs also emit a significant amount of blue light, with both positive and negative effects on the body and the skin. Here, we are presenting a brief literature review on the various mechanisms by which, blue light damages skin as well as various preventative methods. The focus of this article is on the particular cell‐signaling routes involved as well as how the processes at work might be used to treat a range of cutaneous issues.
2 BLUE LIGHT: WHAT IS IT?
Different wavelengths make up all the light that we see. Selected wavelengths exhibit some selected hues. The visible spectrum of light is made up of the colors including red, orange, yellow, green, blue, indigo, and violet. The electromagnetic spectrum's ultraviolet region is closest to blue light, which has the shortest wavelength. These wavelengths have the highest energy and the shortest wavelength, while red light has the least energy and the longest wavelength. Depending on the source, the spectrum of this blue light typically ranges from 420 to 490 nm, with a peak emission between 440 and 460 nm. Infrared light and ultraviolet (UV) light are also two different types of light that have different wavelengths from those found in the visible spectrum.
At homes and inside the commercial buildings, LED lights are becoming more popular and taking the place of incandescent bulbs due to their high efficiency, compact size, and extended lifespan. The main source of blue light is sunlight. There are also synthetic sources, though. Prior to the development of LED lighting, the main source of illumination was incandescent bulbs, which released light with wavelengths comparable to those that the sun naturally emits. Incandescent lighting sources were gradually phased out as the cost of LED lighting continued to drop. Many businesses utilize LED lights in liquid crystal displays (LCDs) and lighting fixtures due to their tiny size, compact design, energy efficiency, and dependability. It has a wide range of uses, including flashes in cameras, smartphones, current computer screens, televisions, smartwatches, and traffic signals. These LEDs also create a good amount of blue light, which is toxic and damaging to the eyes and skin. Concerns about the safety of these light sources have been raised by the fast‐growing use of cellphones, tablets, laptops, and desktop computers, particularly during the COVID‐19 lockdown, when people kept themselves occupied by browsing the Internet and watching televised programs. There is a growing concern about the long‐term consequences, because of the proximity to the screen and the exposure time spent staring at the screen, even if the effects of blue light generated from electronic device screens are fewer than that of sun exposure.
3 WHAT EFFECTS DOES THE BLUE LIGHT HAVE ON YOUR BODY?
The circadian rhythm, or the body's natural sleep cycle, is regulated by blue light. The body's sleep cycle is regulated by exposure to the blue light during the day, which also encourages the generation of melatonin at night. The body's circadian rhythm is hampered by the increased use of gadgets like laptops and phones, even late into the night. The body's capacity to create melatonin is compromised by increasing the amount of blue light exposure before night, which results in difficulty falling asleep and drowsiness during the day.
Blue light improves mood, memory, and cognitive function while increasing alertness. According to studies, youngsters who aren't exposed to enough sunshine may experience problems with the eyes and visual development as well as growth. Research has also suggested that less exposure to blue light may be linked to an increase in myopia.,
High‐intensity blue light, a form of “visible light,” penetrates the skin more deeply than UVB and UVA rays do. Moreover, emerging scientific evidence suggests that the blue light can permanently harm skin cells in the dermis and epidermis. This has the side consequence of damaging the DNA within these cells and stimulating the breakdown of the support fibers for the skin. This may cause fine lines, wrinkles, and premature aging over time.
4 BLUE LIGHT'S MECHANISM OF ACTION
While UVA penetrates deeper layers of the skin and affects immune cells in the epidermis and dermis, UVB interacts with epidermis cells. Visible light penetrates the skin deeper than infrared radiation, while also acting more superficially than UV. The epidermis's hemoglobin and melanin are very effective in absorbing visible light. Blue light can penetrate as far as 0.07 to 1 mm. Endogenous nucleic acids, aromatic amino acids, urocanic acid, tryptophan, tyrosine, NADPH, NADH cofactors, cytochromes, riboflavins, porphyrins, melanin and melanin precursors, protoporphyrin IX, bilirubin, hemoglobin, carotene, or water molecules are examples of chromophores, which are the molecules that absorb the blue light. Consequently, the impact of blue light depends on various chromophores (photo acceptors). Opsins, flavins, porphyrins, and nitrosated proteins are the primary and most significant photo acceptors (e.g., S‐nitro‐albumin).
The activation of flavins and flavoproteins is one such putative blue light pathway. When exposed to radiation, flavin mononucleotides (FMN) and flavin adenine dinucleotides (FAD) double the amount of superoxide that is produced when reactive oxygen species (ROS) are formed. ROS signaling is mediated in a variety of ways. One of these is an Nrf2‐dependent process, which involves the production of antioxidant factors through the action of a “basic leucine zipper protein.” Nrf2 has anti‐inflammatory properties because it inhibits NF‐kB, which controls the proinflammatory response. Flavin‐containing proteins are present in many different types of cells. Cryptochromes are one of these proteins. In a recent study, Buscone et al. hypothesized that blue light via cryptochrome 1 (CRY1), which is found in the hair follicle following exposure to 453 nm light, may have a beneficial influence on hair development. Ex vivo hair follicles showed a lengthening of the anagen phase, which may be related to the rise in CRY1 levels brought on by blue light exposure.,
In the dermis, blue light also causes the release of free nitric oxide NO. At physiological pH, blue light at 420 or 453 nm caused a large amount of NO to develop from S‐nitroso albumin as well as from aqueous nitrite solutions via a Cu(1+)‐dependent process, as measured by chemiluminescence detection (CLD). Blue light irradiation considerably raised the intradermal levels of free NO, as discovered by electron paramagnetic resonance spectrometry in vitro with human skin specimens. Blue light irradiation of human skin resulted in significant NO emanation from the irradiated skin area as well as significant NO translocation from the skin surface into the underlying tissue, as detected by CLD in vivo in healthy volunteers. NO reacts with superoxide to form peroxynitrite, which may cause DNA damage that results in cell damage but no apoptosis has been seen. Yoo et al. discovered that human keratinocyte and cutaneous fibroblast proliferation was inhibited by blue light.
According to some theories, the complex IV of the electron transport chain called cytochrome c oxidase, which is located in the mitochondrial membrane, maybe the mechanism through which blue light influences mitochondrial activity. After being inhibited by NO, Dungel et al. showed that blue light at a wavelength of 430 nm reactivates the mitochondrial respiratory function.
Since blue light activates opsin (OPN), which are G‐protein receptors, their function is also studied. There are various categories of opsins, depending on where they are expressed. In the epidermis, OPN2, OPN3, and OPN4 are expressed. Blue light may activate the opsin receptor, triggering transient receptor potential channels that then release calcium, activating calcium/calmodulin‐dependent protein kinase‐II (CAMKII), which in turn alters gene transcription. OPN2 (Rhodopsin) and OPN3 (Panopsin, Encephalopsin) were discovered to be expressed in the anagen hair follicle in addition to the skin. In an ex vivo study, Buscone et al. showed that blue light irradiation (3.2 J/cm2, 453 nm) lengthened the anagen phase in hair follicles. Opsin's function in controlling melanogenesis and pigmentation has also been studied, although only in Fitzpatrick skin types III and higher. It was discovered that blue light directly affects melanocytes and indirectly affects calcium‐dependent melanogenesis through OPN3. Tyrosinase stimulation occurs in melanocytes of the higher Fitzpatrick phototype as a result of the formation of multimeric tyrosinase, which is triggered by blue light., ,
5 HOW CAN BLUE LIGHT HURT YOUR SKIN?
Several research demonstrate the harmful effects of blue light. According to Dong et al., blue light at 410 nm decreased the transcription of the PER1 gene in keratinocytes. It is a clock gene that plays a role in the circadian rhythm, which may imply that skin cells have the ability to regulate the production of the clock gene in response to light perception. It is hypothesized that blue light would interfere with skin cells' nightly rhythm, which is crucial for skin cell regeneration and repair. Cells may experience the night as being sunlight.
Human skin exposed to blue light may produce free radicals as a result of the decline in carotenoids. It is thought that this oxidative stress on melanogenic precursors causes pigmentation alterations, such as sudden and persistent darkening of the skin. The coloration is consistent and gets darker. It was supported by Melan‐A‐positive cells discovered in skin exposed to blue light. The amount of blue light that is applied to the skin interrupts the function of the melanocytes, causing hyperpigmentation, melasma, and uneven and excessive dark blotches on the skin. However, only people with darker skin tones respond to and show hyperpigmentation from exposure to visible light. The tyrosinase and dopachrome tautomerase protein complex, which is more prevalent in melanocytes seen in darker skin types, can be used to explain this phenomenon. Additionally, blue light increases the production of the proinflammatory cytokine TNF—by activating the activator protein 1 (AP‐1) and nuclear factor b (NF‐B), as demonstrated by Yoo et al. This results in redness and swelling when the same person's skin was exposed to comparable levels of UVA rays.
Roughly speaking, blue light can produce reactive oxygen species. A reactive oxygen species is an unstable molecule that contains oxygen and interacts with other molecules. The primary free radical brought on by exposure to blue light is superoxide (O2), a highly reactive anion radical that is created by the flavins. According to research, the creation of superoxide by blue light may play a substantial role in the aging and carcinogenesis of the skin. Overexposure to ROS can harm skin cells, accelerate aging, cause hyperpigmentation, and cause melisma. By generating DNA damage, these unstable chemicals also cause inflammation and the destruction of the skin's healthy collagen and elastin, which furthers skin laxity, early aging of the skin, and wrinkles. In skin cells, blue light activates the enzyme matrix metalloproteinases (MMPs), which have been shown to break down collagen and speed up the aging process. These MMPs not only break down the existing collagen but also impede the synthesis of new collagen, preventing healing. Antioxidant levels in cells with ROS are also affected. These species are eliminated by antioxidants in the skin, thus after exposure to blue light, they become depleted in the body. It could take up to 24 h for the endogenous repair. Exogenous antioxidants used topically, orally, or both have been found to be advantageous in the case of UV radiation; however, the impact of blue light has not yet been established. The majority of superoxide is quickly changed into hydrogen peroxide. Blue light may not primarily harm cells by overpowering their antioxidant defenses, but rather by continuously producing small amounts of radicals that may slip past the body's regular defenses and harm DNA permanently.
6 THE ADVANTAGES OF BLUE LIGHT
Blue light not only can damage the skin in a number of ways, but it also has certain healing effects. According to the literature, it has been used to cure a variety of skin conditions.
Mild to moderate plaque psoriasis: assistance in the reduction of the redness and the size of the patch without any side effects after a 4‐week treatment term. In their study of the impact of blue light on keratinocytes, Becker et al. found that the proliferation of these cells decreased with exposure time, with a reduction in keratinocyte proliferation being seen after 15 min of irradiation. Another potential reason for a decrease in keratinocyte proliferation is nitric oxide (NO)‐mediated beginning of keratinocyte differentiation.,
Atopic Dermatitis: Blue light therapy for atopic dermatitis and eczema revealed a 54% reduction in the disease severity following a 6‐month treatment period. ROS signaling is mediated in a variety of ways. One of these is an Nrf2‐dependent process, which involves the production of antioxidant factors through the action of a “basic leucine zipper protein.” Nrf2 has anti‐inflammatory properties, because it inhibits NF‐kB, which controls the proinflammatory response.
Acne: Reduced number of open and closed comedones has been observed in mild to moderate acne. The primary theory postulates that the beneficial effect is connected to a decrease in Propionibacterium acnes follicular colonization, which may be related to the activation of endogenous bacterial porphyrins by blue light. Blue and red light may prevent sebocytes from producing lipids, which suggests that treating acne by preventing sebum production could be beneficial.,
Photodynamic treatment: Another medical application of the blue light is regarding the photodynamic treatment, which uses a photosensitizing chemical along with light and oxygen to produce highly reactive singlet oxygen and treat some cancer‐causing and noncancerous skin disorders. Aminolevulinic acid (ALA) and blue light are frequently used for the treatment of proliferative and inflammatory diseases of the skin. When performed properly, photodynamic treatment using blue light for photorejuvenation is thought to be both efficient and secure. The use of photodynamic therapy and other blue light therapies is currently being used in the clinics.
7 HOW TO AVOID POTENTIAL SKIN DAMAGE FROM THE BLUE LIGHT
The best treatment is prevention. It is more crucial to try to take preventative measures through various treatment. The simplest approach to minimize blue light damage is to restrict exposure and reduce screen time by taking frequent pauses from your device to rest your eyes. Attempt to take five‐minute rests every 30 min. Invest in blue light screen filters or screen protectors for your electronic devices (such as a phone, tablet, or computer), which can block or tame blue light. Numerous businesses have created blue light‐blocking eyewear that makes the same claims about improving sleep and reducing eye strain. The effectiveness of these lenses is still up for question among scientists, despite the fact that laboratory tests indicate that they should be beneficial. To decrease the emission of the blue light, switch your computer, smartphone, and other devices into “night mode”., The amount of blue light emitted by screen technology is influenced by several variables, including program code, the mobile operating system, and screen engineering (Calvo‐Sanz & Tapia‐Ayuga, 2020). Melatonin levels were inhibited with all types of lightning, according to a study evaluating the effectiveness of a program published by Apple Inc. termed “night‐shift” mode settings on iPad 2019. Therefore, it is suggested to decrease all types of lightning as well as blue light over nights to decrease the suppression of melatonin.
Headphones can be used so the phone can be kept in the pocket and away from your cheek and face.
Observe the 20‐20‐20 Rule: Spend 20 min looking at a screen, then 20 s looking at something 20 feet away.
8 SUNSCREEN
People should always wear sunscreen every day. Unfortunately, not all sunscreens offer blue light protection. TiO2 (a component in physical sunscreen) has been determined to have blue light blocking properties based on several assessments.
Physical and chemical sunscreens are the two primary categories of sunscreens. Physical sunscreens have active, physical components that are iron oxide, tungsten dioxide, zinc oxide and many more. Other ingredients include talc, red veterinary petrolatum, kaolin, calamine, and iron oxide. By reflecting, dispersing, or absorbing UV radiation, inorganic materials work. Their inherent drawbacks of being opaque and having a “whitening effect” can be lessened by using micronized or ultrafine particles. As soon as its applied, it rests on top of the skin. Physical sunscreens do provide blue light protection since the ingredients is made to reflect UV and blue light away from the skin. Chemical compounds that really absorb UV rays and may even hurt the skin are used to make chemical sunscreens. Blue light protection is not provided by chemical sunscreens.,
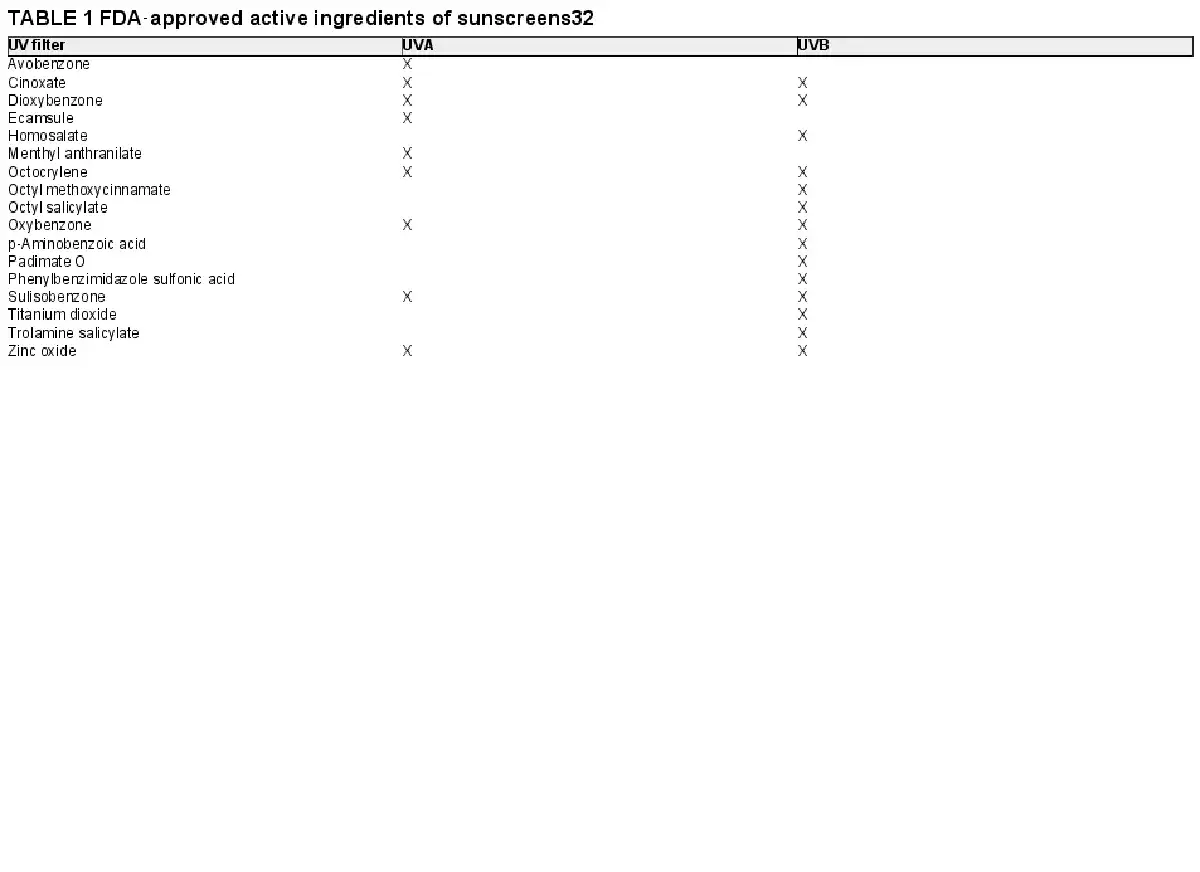
Additionally, a number of substances—often referred to as “systemic sunscreens”—have a systemic photoprotective action like green tea polyphenols, PABA, antihistamines, aspirin, indomethacin, corticosteroids, beta‐carotene, antimalarials, ascorbic acid, and tocopherols (i.e., vitamins A, C, and E) (Table 1).,
9 ANTIOXIDANTS
The development of ROS is one of blue light exposure's most harmful side effects. Fortunately, antioxidants are substances that, by neutralizing reactive oxygen species in biological tissues, can halt oxidative chain reactions and postpone oxidative damage (Gülçin, 2010). It was found in a study by Bapary et al. (2019) that antioxidants and a drop in ROS were directly correlated, supporting the idea that antioxidants have ROS lowering properties.
The skin makes use of a variety of antioxidative defense mechanisms, including the enzymes catalase and superoxide dismutase as well as natural products like L‐ascorbate, beta‐carotene, and glutathione, to control the production of ROS.
A diet high in antioxidants, including fruits and vegetables, is strongly advised in addition to topical application of antioxidant‐rich products. This is the healthiest and most long‐lasting method of avoiding blue light harm to the skin.
Oral antioxidants, such as supplements of the vitamins C and E and glutathione, since all antioxidants work to scavenge free radicals.
The diet should include foods high in antioxidants like fresh fruits and vegetables like beans, spinach, beets, strawberries, blues, and raspberries, which can help the skin fight off free radicals. Plants produce red, orange, and yellow carotenoids, which have antioxidant characteristics. Carotene, lutein, zeaxanthin, and lycopene are a few typical carotenoids. Beta‐carotene can be obtained in diet by eating dark green, red, yellow, and orange vegetables like spinach and carrots. The carrot root and extract, as well as a subtropical fruit extract, both contain carotene and are available as topical ingredients. Another carotenoid called lutein, which makes up a large portion of the macular pigment, is renowned for its capacity to block blue light. As was already noted, vitamins are also often used as ingredients in blue light protection products. Niacinamide, often known as vitamin B3, has been demonstrated to be helpful against hyperpigmentation brought on by aging. Niacinamide is a fantastic option to boost the protection of sunscreens in the visible spectrum. Vitamins C and E are well‐known for their antioxidant properties, and research has shown that these two nutrients can shield the skin against UVA rays. These vitamins may also be helpful against blue light because UVA and blue light are close neighbors on the light spectrum.,
10 CONCLUSION
The majority of frequently used electronic devices, including smartphones, computers, and other devices, generate blue light. The wavelength and intensity of blue light exposure have been proved to have a significant impact on the skin's reaction. In many dermatological illnesses, it has a curative impact with minimal exposure; on the other hand, long‐term exposure has numerous detrimental effects, including DNA damage, oxidative stress, increased melanogenesis leading to pigmentation, photoaging, etc. In the near future, as we learn more about the mechanism of harm that blue light exposure causes to the skin, we may anticipate seeing a rise in the number of compounds introduced for blue light protection and new methodologies created to test goods for blue light protection claims. People who are frequently exposed to blue light pollution must take various precautionary steps because exposure to blue light is inevitable.
AUTHOR CONTRIBUTIONS
Jyoti Kumari: Writing and revising the manuscript. Kinnor Das, Mahsa Babaei, and Ghasem Rahmatpour Rokni: Review and revising the manuscript. Mohamad Goldust: Conception, writing, review, and revising the manuscript
CONFLICT OF INTEREST
None.
DISCLAIMER
We confirm that the manuscript has been read and approved by all the authors, that the requirements for authorship as stated earlier in this document have been met and that each author believes that the manuscript represents honest work.
ETHICAL APPROVAL
No ethical approval was required as this research did not involve human subjects or animals.
REFERENCES
- 1. Coats JG, Maktabi B, Abou‐Dahech MS, Baki G. Blue light protection, part I—effects of blue light on the skin. J Cosmet Dermatol. 2021;20(3):714–717.
- 2. Tosini G, Ferguson I, Tsubota K. Effects of blue light on the circadian system and eye physiology. Mol Vis. 2016;22:61–72.
- 3. O'Hagan JB, Khazova M, Price LLA. Low‐energy light bulbs, computers, tablets and the blue light hazard. Eye. 2016;30(2):230–233.
- 4. Jakhar D, Kaul S, Kaur I. Increased usage of smartphones during COVID‐19: is that blue light causing skin damage? J Cosmet Dermatol. 2020;19(10):2466–2467.
- 5. Dong K, Goyarts EC, Pelle E, Trivero J, Pernodet N. Blue light disrupts the circadian rhythm and create damage in skin cells. Int J Cosmet Sci. 2019;41(6):558–562.
- 6. Alkozei A, Smith R, Dailey NS, Bajaj S, Killgore WDS. Acute exposure to blue wavelength light during memory consolidation improves verbal memory performance. PLoS One. 2017;12(9):e0184884.
- 7. Alkozei A, Smith R, Pisner DA, et al. Exposure to blue light increases subsequent functional activation of the prefrontal cortex during performance of a working memory task. Sleep. 2016;39(9):1671–1680.
- 8. D'Orazio J, Jarrett S, Amaro‐Ortiz A, Scott T. UV radiation and the skin. Int J Mol Sci. 2013;14(6):12222–12248.
- 9. Sowa P, Rutkowska‐Talipska J, Rutkowski K, Kosztyła‐Hojna B, Rutkowski R. Optical radiation in modern medicine. Postepy Dermatol Alergol. 2013;30(4):246–251.
- 10. Yang MY, Chang CJ, Chen LY. Blue light induced reactive oxygen species from flavin mononucleotide and flavin adenine dinucleotide on lethality of HeLa cells. J Photochem Photobiol B. 2017;173:325–332.
- 11. Buscone S, Mardaryev AN, Westgate GE, Uzunbajakava NE, Botchkareva NV. Cryptochrome 1 is modulated by blue light in human keratinocytes and exerts positive impact on human hair growth. Exp Dermatol. 2021;30(2):271–277.
- 12. Garza ZCF, Born M, Hilbers PAJ, van Riel NAW, Liebmann J. Visible blue light therapy: molecular mechanisms and therapeutic opportunities. Curr Med Chem. 2018;25(40):5564–5577.
- 13. Yoo JA, Yu E, Park SH, et al. Blue light irradiation induces human keratinocyte cell damage via transient receptor potential vanilloid 1 (TRPV1) regulation. Oxid Med Cell Longev. 2020;2020:e8871745.
- 14. Dungel P, Haindl S, Redl H, Kozlov AV. O20. low level light illumination reactivates mitochondria inhibited by nitric oxide in a wavelength dependent manner. Nitric Oxide. 2008;19:24.
- 15. Serrage H, Heiskanen V, Palin WM, et al. Under the spotlight: mechanisms of photobiomodulation concentrating on blue and green light. Photochem Photobiol Sci. 2019;18(8):1877–1909.
- 16. Buscone S, Mardaryev AN, Raafs B, et al. A new path in defining light parameters for hair growth: discovery and modulation of photoreceptors in human hair follicle. Lasers Surg Med. 2017;49(7):705–718.
- 17. Regazzetti C, Sormani L, Debayle D, et al. Melanocytes sense blue light and regulate pigmentation through opsin‐3. J Invest Dermatol. 2018;138:171–178.
- 18. Campiche R, Curpen SJ, Lutchmanen‐Kolanthan V, et al. Pigmentation effects of blue light irradiation on skin and how to protect against them. Int J Cosmet Sci. 2020;42(4):399–406.
- 19. Becker A, Sticht C, Dweep H, van Abeelen FA, Gretz N, Oversluizen G. Impact of blue LED irradiation on proliferation and gene expression of cultured human keratinocytes. In: mechanisms for low‐light therapy X [internet]. SPIE; 2015:58–69. Available from: https://www.spiedigitallibrary.org/conference‐proceedings‐of‐spie/9309/930909/Impact‐of‐blue‐LED‐irradiation‐on‐proliferation‐and‐gene‐expression/10.1117/12.2083010.full. [cited 2022 Aug 11].
- 20. Weinstabl A, Hoff‐Lesch S, Merk HF, von Felbert V. Prospective randomized study on the efficacy of blue light in the treatment of psoriasis vulgaris. Dermatology. 2011;223(3):251–259.
- 21. Becker D, Langer E, Seemann M, et al. Clinical efficacy of blue light full body irradiation as treatment option for severe atopic dermatitis. PLoS One. 2011;6(6):e20566.
- 22. Tzung TY, Wu KH, Huang ML. Blue light phototherapy in the treatment of acne. Photodermatol Photoimmunol Photomed. 2004;20(5):266–269.
- 23. Scott AM, Stehlik P, Clark J, et al. Blue‐light therapy for acne vulgaris: a systematic review and meta‐analysis. Ann Fam Med. 2019;17(6):545–553.
- 24. Yin R, Dai T, Avci P, et al. Light based anti‐infectives: ultraviolet C irradiation, photodynamic therapy, blue light, and beyond. Curr Opin Pharmacol. 2013;13(5):731–762.
- 25. Coats JG, Maktabi B, Abou‐Dahech MS, Baki G. Blue light protection, part II—ingredients and performance testing methods. J Cosmet Dermatol. 2021;20(3):718–723.
- 26. Calvo‐Sanz J a, Tapia‐Ayuga CE. Blue light emission spectra of popular mobile devices: the extent of user protection against melatonin suppression by built‐in screen technology and light filtering software systems. Chronobiol Int. 2020;37(7):1016–1022.
- 27. Nagare R, Plitnick B, Figueiro M. Does the iPad night shift mode reduce melatonin suppression? Light Res Technol Lond Engl 2001. 2019;51(3):373–383.
- 28. Brian CO. Deconstructing the 20‐20‐20 rule for digital eye strain. Optom Times. 2018;10(3):21–23.
- 29. Chunnawong O, Pitaksuteepong T. The Development and Evaluation of the Sunscreen Product for UV‐Visible Protection. Naresuan University; 2019 [PhD Thesis].
- 30. Pa NP, Highton A, Moy RL. Properties of topical sunscreen formulations: a review. J Dermatol Surg Oncol. 1992;18(4):316–320.
- 31. O'Donoghue MN. Sunscreen: the ultimate cosmetic. Dermatol Clin. 1991;9:99–104.
- 32. Pirotta G. Sunscreen regulation in the world. In: Tovar‐Sánchez A, Sánchez‐Quiles D, Blasco J, eds. Sunscreens in Coastal Ecosystems: Occurrence, Behavior, Effect and Risk [Internet]. Springer International Publishing; 2020:15–35. (The Handbook of Environmental Chemistry): Accessed 10 Aug, 2022. doi:10.1007/698_2019_440
- 33. Sambandan DR, Ratner D. Sunscreens: an overview and update. J Am Acad Dermatol. 2011;64(4):748–758.
- 34. Pathak MA. Sunscreens: topical and systemic approaches for protection of human skin against harmful effects of solar radiation. J Am Acad Dermatol. 1982;7(3):285–312.
- 35. Gulcin İ. Antioxidants and antioxidant methods: an updated overview. Arch Toxicol. 2020;94(3):651–715.
- 36. Bapary MAJ, Takano J, Soma S, Sankai T. Effect of blue light‐emitting diode light and antioxidant potential in a somatic cell. Cell Biol Int. 2019;43(11):1296–1306.
- 37. Sadowska M, Narbutt J, Lesiak A. Blue light in dermatology. Life. 2021;11(7):670.