Introduction
Tube insertion of glaucoma drainage devices in pediatric cases may be challenging due to abnormal anterior segment anatomy complicating placement, and corneal opacities limiting visualization. These complexities may lead to complications such as poorly placed tubes and leakage from inadvertent tract expansion. Postoperative tube-related complications include clogs, kinks, identification of inadvertent cuts, or retraction. In the context of pediatric glaucoma, where patients may undergo initial glaucoma drainage device placement early in life, ocular growth and aggressive scarring may also cause tube retraction outside of the anterior chamber necessitating tube replacement or extension. Similar to initial glaucoma drainage device tube placement, tube extension in pediatric cases may be complicated by complex anatomy and limited visualization. In this article, we discuss surgical techniques for initial non-valved glaucoma drainage device tube placement and a glaucoma drainage device tube extension using polypropylene suture as a guidewire and stabilizer in pediatric patient populations.
Technique
Tube Placement
Materials for this technique include a nonvalved glaucoma drainage device implant and a blue 3-0 polypropylene (Ethicon) suture. After dissecting the Tenon capsule and conjunctiva, the glaucoma drainage device reservoir is sutured to the sclera in a standard manner. Estimating the length of the desired tract, the tube is cut accordingly. Starting from the endplate side, a blue 3-0 polypropylene suture is threaded through the glaucoma drainage device tube's lumen until it passes through completely to the tube's open end (Figure 1A). A 23-gauge needle is used to create a sclerostomy tract approximately 3 to 4 mm posterior to the limbus to the tube's desired end position in the anterior segment (Figure 1B). In some circumstances, this may require passing through high iris insertion or synechiae adhesions. The polypropylene tip protruding from the free end of the glaucoma drainage device tube is passed through the previously made sclerostomy tract (Figure 1C). The blue color of the polypropylene material allows for easier visualization in the anterior chamber. The rigid polypropylene filament passes with ease through fibrinous obstacles and the iris. If the polypropylene suture encounters resistance while being passed through the sclerostomy tract, the suture can be removed and cut at an angle to create a beveled tip. Once the tip of the polypropylene filament can be visualized in the desired area in the anterior chamber, the tube is then advanced along the polypropylene until its end position in the anterior chamber is reached. Once tube placement is appropriate, the guidewire suture is removed from the tube's lumen closest to the endplate (Figure 1D). Alternatively, according to the surgeon's discretion, a paracentesis can be created and the polypropylene can be removed from the tube's distal end using intraocular forceps. The remainder of the surgery (verification of tube patency, ligation and confirmation of ligation, and tube attachment to episcleral tissue) can be performed following surgeon preference.
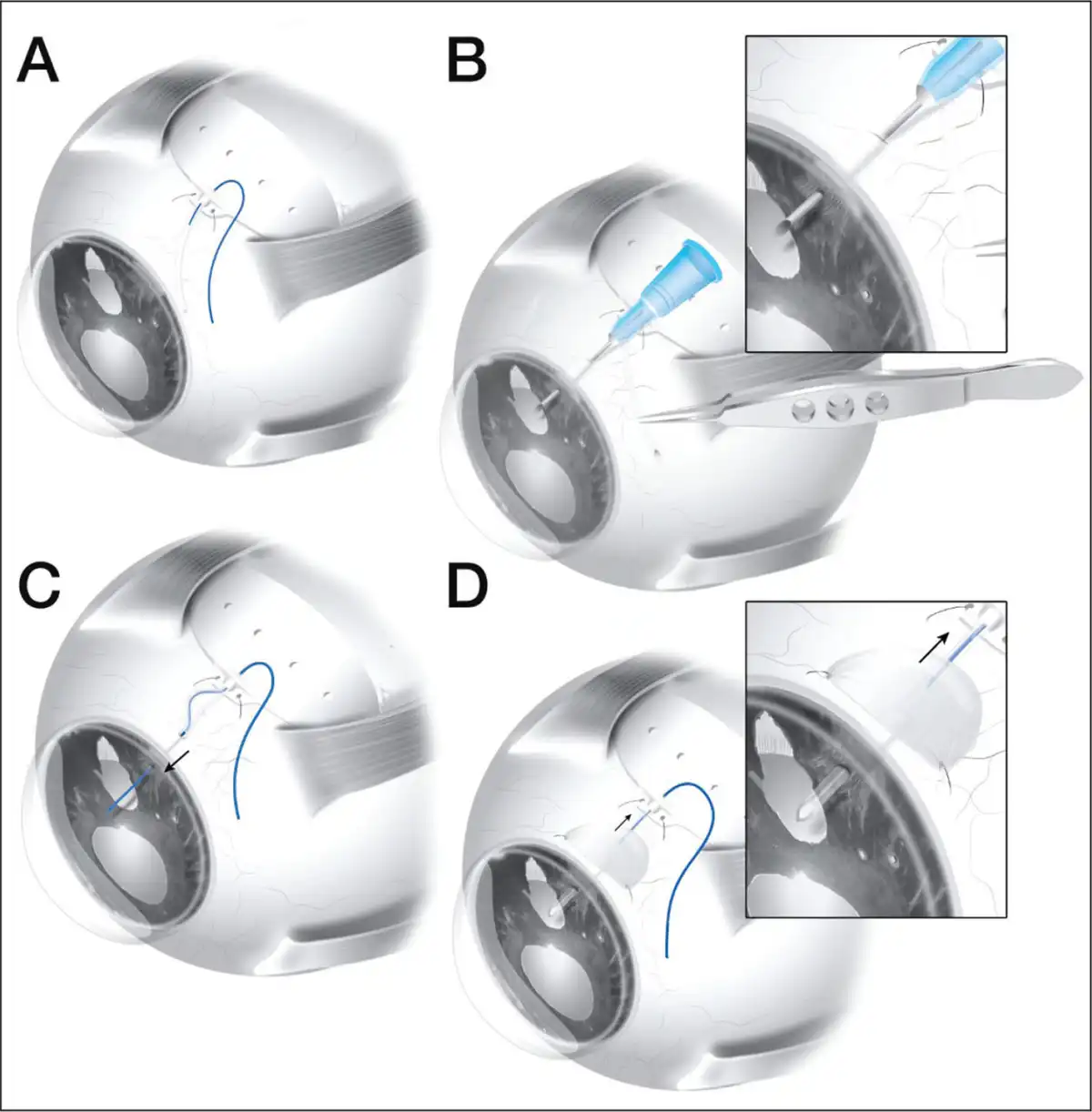
Figure 1
Polypropylene-assisted tube insertion. (A) Insertion of polypropylene through the tube's distal end. (B) Creation of sclerostomy tract using a 23-gauge needle from 3 to 4 mm posterior to the limbus to desired end position in the anterior segment. (C) Threading of polypropylene through sclerostomy tract prior to sliding the tube over polypropylene guidewire. (D) Removal of polypropylene after ideal placement of the tube.
Tube Extension
Once the existing tube is identified, the over-lying tissues are dissected until the tube is exposed and, if necessary, externalized. After flushing a balanced salt solution into the existing tube to expand the plate capsule, a blue 3-0 polypropylene can be threaded through the lumen until there is resistance at the endplate. Tube extension can be assisted with polypropylene when using an additional glaucoma drainage device tube, angiocatheter, or alternative tubes such as a nasolacrimal stent. Methods to prepare the extending tube include cutting a 1-mm slit parallel to the tube's length or stretching one end of the extending tube's lumen with Kelman-McPherson forceps. The exposed end of the 3-0 polypropylene should be passed through the extending tube's lumen at the prepared end. With the polypropylene suture stabilizing the two tubes, smooth forceps can be used to assist in sliding the extending tube over the existing glaucoma drainage device tube, ensuring the polypropylene suture emerges fully from the distal end of the extending tube. Once the tubes are securely connected, the extending tube should be cut to the desired length. The polypropylene suture may be removed by pulling at the distal end or, alternatively, can be used to guide placement of the tube in the anterior chamber using the method described above. If using the latter approach, the polypropylene cannot be removed from the endplate without opening the capsule, in which case removal from an alternative paracentesis site may be preferred.
Results
The use of a 3-0 polypropylene suture facilitates efficient placement and extension of glaucoma drainage device tubes using the two methods above. The method described for glaucoma drainage device tube placement is especially useful for pediatric cases with obscure or distorted anatomy and/or limited visualization of the anterior chamber. As opposed to the flexible nature of the silicone tube alone, the polypropylene's rigidity and small diameter allows passage of the suture through the tract without interference from obstructing anatomy such as the iris or fibrous membrane. Furthermore, if using blue polypropylene, the color allows visualization in the anterior chamber despite poor corneal clarity. For tube extension, the rigid structure of the polypropylene suture stabilizes both the extending and existing tubes when sliding one on top of the other. Without the stability of the suture, forceps-assisted guidance of one flexible tube over another flexible tube is difficult.
Discussion
These techniques may solve difficulties with ideal tube placement and simplify tube extension in complex pediatric cases. Wright et al described a similar procedure to the aforementioned glaucoma drainage device tube placement technique but did not emphasize its utility in pediatric patients with complex anterior segment anatomy. Additionally, Andrew et al described a technique for inserting a 3-0 Supramid (S. Jackson, Inc) suture inside the glaucoma drainage device tube's lumen to increase tube rigidity. However, they opted to keep the suture inserted and only remove it postoperatively during a minor procedure if further intraocular pressure lowering was desired. We believe removal of the suture intraoperatively is preferred to optimize the functionality of the glaucoma drainage device and prevent complications, such as endophthalmitis, associated with stent exposure if the suture is removed postoperatively.
The second technique, polypropylene-assisted tube extension, is an alternative approach to a solution for some postoperative glaucoma drainage device tube complications, such as a cut tube or tube retraction. In these cases, the decision to replace or move the entire glaucoma drainage device requires extensive tissue dissection, which runs a risk of impinging on proximal anatomy such as the limbus. By opting to extend the tube rather than replace the glaucoma drainage device implant, the endplate and surrounding capsule can be preserved, maintaining aqueous flow. Although many authors have discussed methods of tube extension, none have used polypropylene to assist with attachment and placement. A previously described technique for tube extension is tube-intube, which can be achieved using materials such as a 22-gauge angiocatheter, additional glaucoma drainage device tube, or alternative tubes such as a nasolacrimal stent. Alternatively, a Tube Extender (New World Medical, Inc), which includes an additional silicone plate and tube with an opening to insert the shortened tube, has also been described by Sarkisian and Netland but can be too long or bulky in a child's eye. Although these previously described extension techniques have been successful in extending the utility of glaucoma drainage device tubes, they do not include the use of a polypropylene suture to facilitate and guide attachment as described here.
Limitations of the use of polypropylene for placement and extension of the glaucoma drainage device tube must be considered. Ligating the tube after placement using polypropylene prevents the surgeon from checking for watertight ligation by flushing. In terms of cost, polypropylene sutures are inexpensive and thus do not add significantly to the cost of placement or extension of glaucoma drainage device tubes.
Overall, using polypropylene as a guidewire and/or stabilizer can facilitate glaucoma drainage device tube placement and extension operations in complex pediatric cases with obscure anatomy, poor visualization, or tube retraction. Future studies may be conducted to confirm the advantages of the described techniques by evaluating procedure times, postoperative intraocular pressures, and postoperative complications.
The authors thank Dr. Aristomenis Thanos, MD, for his illustration services and The Samuel & Ethel Balkan International Pediatric Glaucoma Center for its philanthropic support in the production of this manuscript
References
- 1. Elshatory YM, Gauger EH, Kwon YH, et al. Management of pediatric aphakic glaucoma with vitrectomy and tube shunts. J Pediatr Ophthalmol Strabismus. 2016;53(6):339–343–. PMID:
- 2. Autrata R, Helmanova I, Oslejskova H, Vondracek P, Rehurek J. Glaucoma drainage implants in the treatment of refractory glaucoma in pediatric patients. Eur J Ophthalmol. 2007;17(6):928–937–. PMID:
- 3. Wright MM, Singh K, Grajewski AL. Polypropylene suture stent for insertion of glaucoma tube shunt implants. Ophthalmic Surg. 1994;25(10):743–744–. PMID:
- 4. Team TAAGFID project team. Experimental flow studies in glaucoma drainage device development. Br J Ophthalmol. 2001;85(10):1231–1236–. PMID:
- 5. Sarkisian SR, Netland PA. Tube extender for revision of glaucoma drainage implants. J Glaucoma. 2007;16(7):637–639–. PMID:
- 6. Bansal A, Fenerty CH. Extension of retracted glaucoma drainage tube using a 22-gauge intravenous catheter in complex pediatric glaucoma. J Glaucoma. 2010;19(4):248–251–. PMID:
- 7. Sternfeld A, Dotan G, Bohra L, Roarty J. Ahmed valve tube extension in pediatric glaucoma. J Glaucoma. 2020;29(4):276–279–. PMID:
- 8. Chiang MY-M, Camuglia JE, Khaw PT. A novel method of extending glaucoma drainage tube: “tube-in-tube” technique. J Glaucoma. 2017;26(2):93–95–. PMID:
- 9. Andrew NH, Huang SG, Craig JE. A modified technique for intraluminal stenting of glaucoma drainage devices: the guide-wire technique. Indian J Ophthalmol. 2020;68(6):1151–1153–. PMID:
- 10. Kwon HJ, Kerr NM, Ruddle JB, Ang GS. Endophthalmitis associated with glaucoma shunt intraluminal stent exposure. J Curr Glaucoma Pract. 2016;10(1):36–37–. PMID:
- 11. Porter A, Lee GA, Shah P, Todd B. Glaucoma drainage device tube extension without the need for a tube extender device or angiocatheter. Clin Exp Ophthalmol. 2017;45(3):308–310–. PMID:
- 12. Pandav SS, Gautam N, Thattaruthody F. Tube-in-tube: a solution for retracted tube. J Curr Glaucoma Pract. 2021;15(1):44–46–. PMID:
- 13. Moghimi S, Mohammadi M. Extension of a retracted ciliary sulcus tube of Ahmed glaucoma implant with angiocatheter segment. Int Ophthalmol. 2012;32(4):409–412–.
- 14. Vergados A, Mohite AA, Sung VCT. Ab interno tube ligation for refractory hypotony following non-valved glaucoma drainage device implantation. Graefes Arch Clin Experiment Ophthalmol. 2019;257(10):2271–2278–.