Introduction
The World Health Organization (WHO) reports that cardiovascular diseases (CVDs) contribute to 17.5 million deaths per year. Coronary artery disease (CAD) is a condition of narrowing of the coronary artery that supplies blood to myocardium. Most common cause of which is atherosclerosis (accumulation of fat/cholesterol in the arterial wall). Management of CAD is either medical or surgical procedures. Coronary artery bypass graft (CABG) is performed for both symptomatic and prognostic reasons. The surgery benefits with respect to survival, improved ventricular function, freedom from angina, and re-stenosis. CABG was first performed in India in 1975. Presently the annual number is about 60,000. In a contemporary study of 3500 patients undergoing CABG, 75% had 3 vessel disease, 10% had left main, 25% had severe left ventricle (LV) dysfunction, and 9% had carotid stenosis. The Indian heart weighs less about 100 g compared to in Europid men and women. Asian Indians have a higher operative and overall mortality following coronary bypass surgery. They also have higher rates of post-operative complications and repeat surgeries. In the absence of a central registry, the exact numbers may not be apparent.
Relation Between Sexual Function and CAD
Research suggests the importance of maintaining sexual health for the wellbeing of the cardiovascular system. The correlation between erectile dysfunction (ED) and CAD has been emphasized and ED has been recognized as a potential independent risk factor for prediction of CAD. Evidence is accumulating to support the concept that ED and CAD are differing manifestations of a common underlying vascular pathology. The link between ED and CVD has been postulated both at the pathophysiological and clinical levels. The physiology of sustaining normal erections is a neurovascular phenomenon under the influence of psychological control.
Similar to male erections, female genital arousal is achieved when there is increased blood flow to the labia by vasodilatation, which is accompanied by vaginal lubrication and clitoral erection. studies have also revealed an effect of CVD on women’s sexual desire; arousal dysfunction, with decreased sensitivity of the clitoris and vaginal labia; and orgasm.-
Studying the epidemiology of sexual dysfunctions becomes difficult as the frequency of reporting and seeking help varies, the reasons vary from knowledge and attitude about the problem to social and cultural upbringing of the individual. Sexuality in elderly is one of the neglected topics and it is also associated with lots of myths and misconceptions. Studies have shown that sexual dysfunctions increase with age and the prevalence increases further with the presence of comorbidities like chronic medical illnesses. Studies on the practice of sex in elderly are few more, particularly in cardiac patients. The current study is an attempt to understand the depth of the relation between cardiovascular illness and sexual functioning in an individual and also to assess the persons presenting with sexual dysfunction for detailed evaluation of CVDs for better outcomes.
Materials and Methods
The study is a cross-sectional study of descriptive and explorative design, conducted at JSS Hospital, JSS University, Mysuru, which is a tertiary care center drawing patients from nearly 18 districts. The source of data was collected from the Department of Cardiovascular Sciences, JSS Hospital, Mysuru.
Initially, 57 patients were considered for the study; later because of the mortality, the final number of individuals considered was 54. Individuals diagnosed with ischemic heart disease (IHD), acute coronary syndromes, and triple vessel disease were included for the study. The diagnosis was made by the concerned ECG changes and cardiac biomarkers, and confirmed by the attending cardiologist. The interview was conducted once the patient was stabilized and was physically fit to participate in the study and before discharge.
Inclusion Criteria
Patients diagnosed with CAD and those who have undergone cardio-thoracic intervention and are capable of participating in the study after review by the cardiologist/surgeon in charge.
Age 18 and above, both male and female.
Exclusion Criteria
Patients who refuse to give consent.
Patients who are not able to participate in the interviews.
Patients who are considered unfit to participate by the cardiologist/surgeon in charge.
Written informed consent was taken from the subjects. They were informed about the study. Adequate privacy and confidentiality were ensured. The sociodemographic details were collected along with contact details. Adequate privacy was maintained during the interview, to make sure that the patient feels comfortable and gives details without hesitancy. Sexual functioning was assessed using structured and validated pro forma. For men, International Index for Erectile Functioning (IIEF) and for women Female Sexual Function Index (FSFI), was used.
Statistical Analysis
Descriptive and inferential statistical analysis has been carried out in the present study. Results on continuous measurements are presented on Mean ± SD (Min-Max) and results on categorical measurements are presented in number (%). Significance is assessed at 5% level of significance. ANOVA and Student’s t test, statistical software SAS 9.2, SPSS 15.0, Stata 10.1, MedCalc 9.0.1, Systat 12.0 and R environment ver.2.11.1 were used for statistical analysis.
Results
Sociodemographic Details
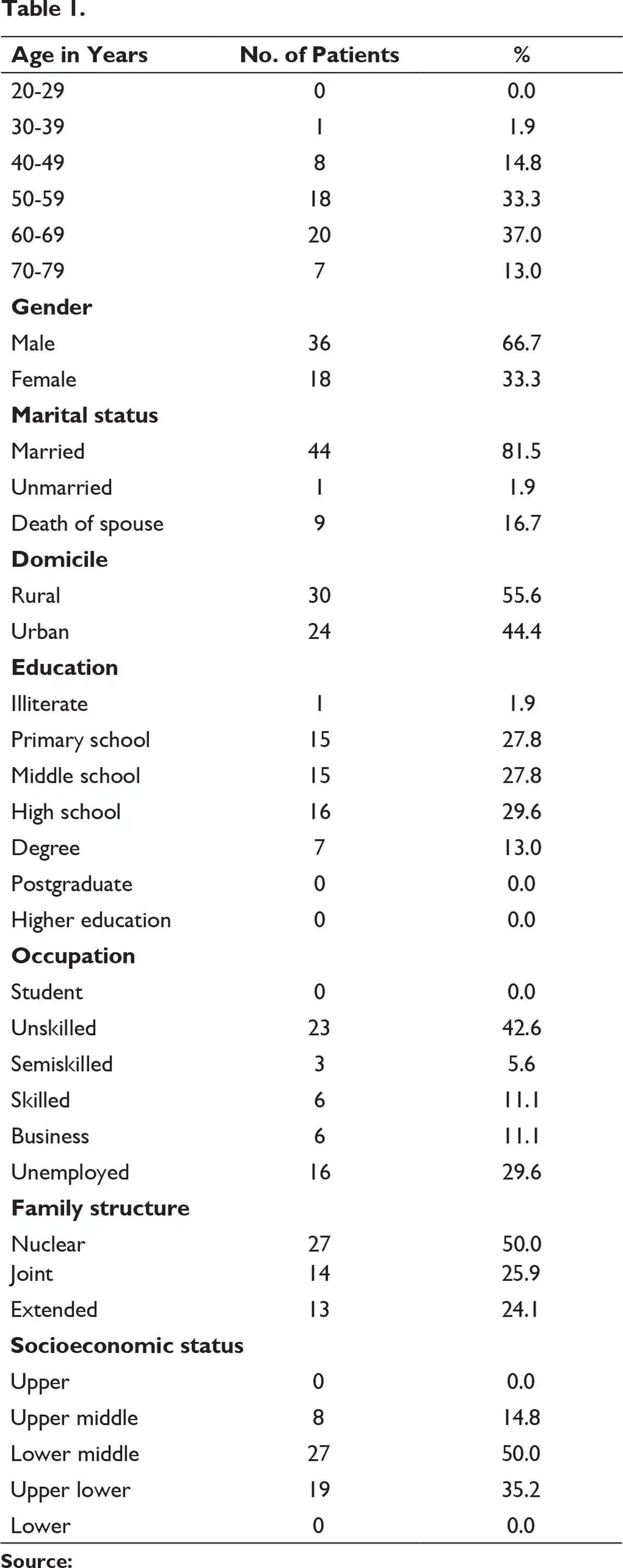
The total study sample was 54 patients including both males and females. Males were the predominant sex constituting about 66.7% of the total sample. A wide range of age group was selected to assess the prevalence of sexual dysfunction in the population. Majority of the study group was between 50 and 70 years (70.3%), married people (81.5%), followed by single widowed individuals (16.7%). Nearly 81.5% were married, 16.7% were widow/widowers. Almost 56% were hailing from a rural background. Majority had attended high school (29.6%) and were working as unskilled laborers (42.6%). Nuclear family (50 %) was on the rise and the number of family members constituted 5-6 in 46.3% of patients. Lower middle socioeconomic class constituted 50% followed by upper lower (35.2%) class depicted in Table 1.
Risk Factor Profile
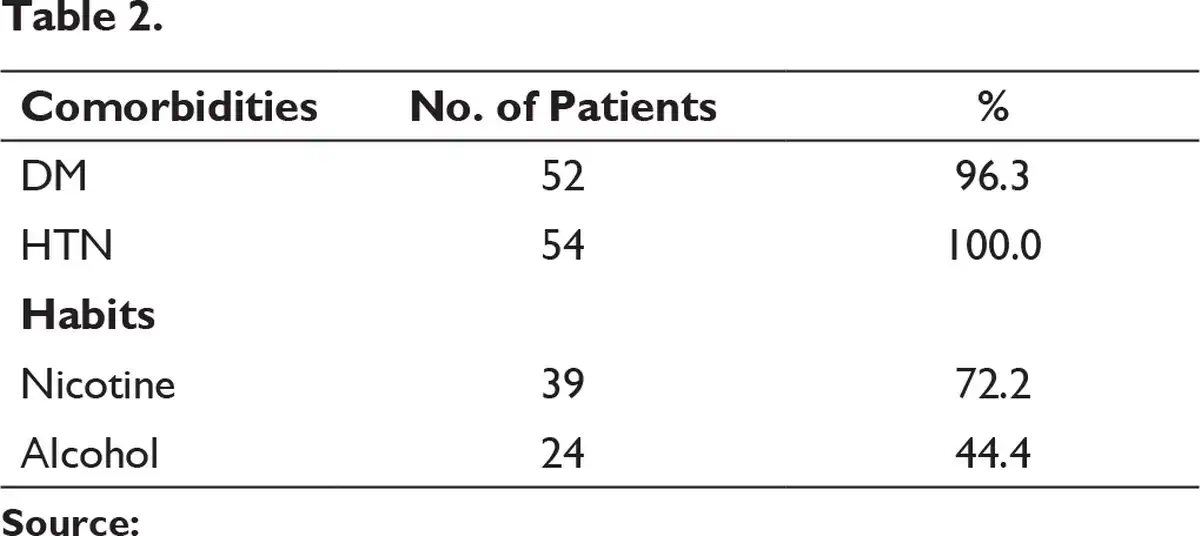
Diabetes mellitus and hypertension were associated with 96.3% and 100%, respectively, that is, all the study subjects were hypertensives. Alcohol and nicotine consumption was associated with 44.4% and 72.2% individuals, respectively (Table 2). All the individuals had positive family history of medical conditions.
Profile for CABG Surgery
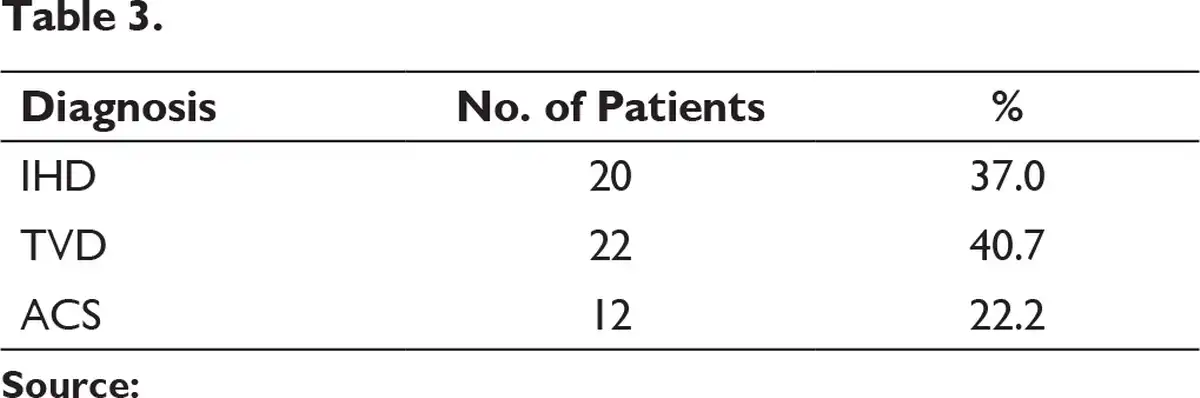
Triple vessel disease (40.7%) was the most common indication for CABG, followed by IHD (30.7%) and acute coronary syndromes (ACS; 22.2%) (Table 3).
Abbreviations: IHD, ischemic heart disease; TVD, triple vessel disease; ACS, acute coronary syndrome.
Sexual Dysfunction
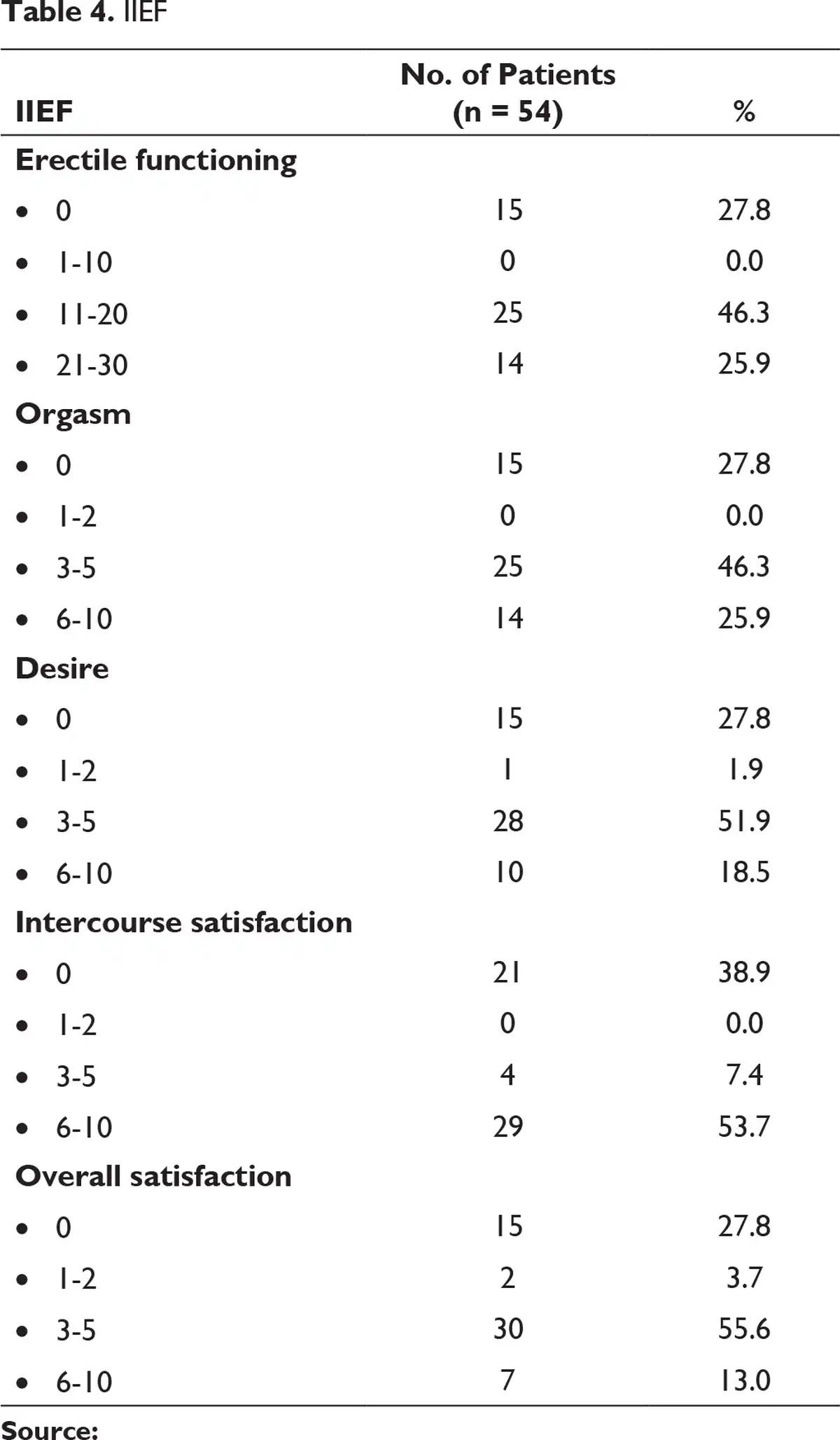
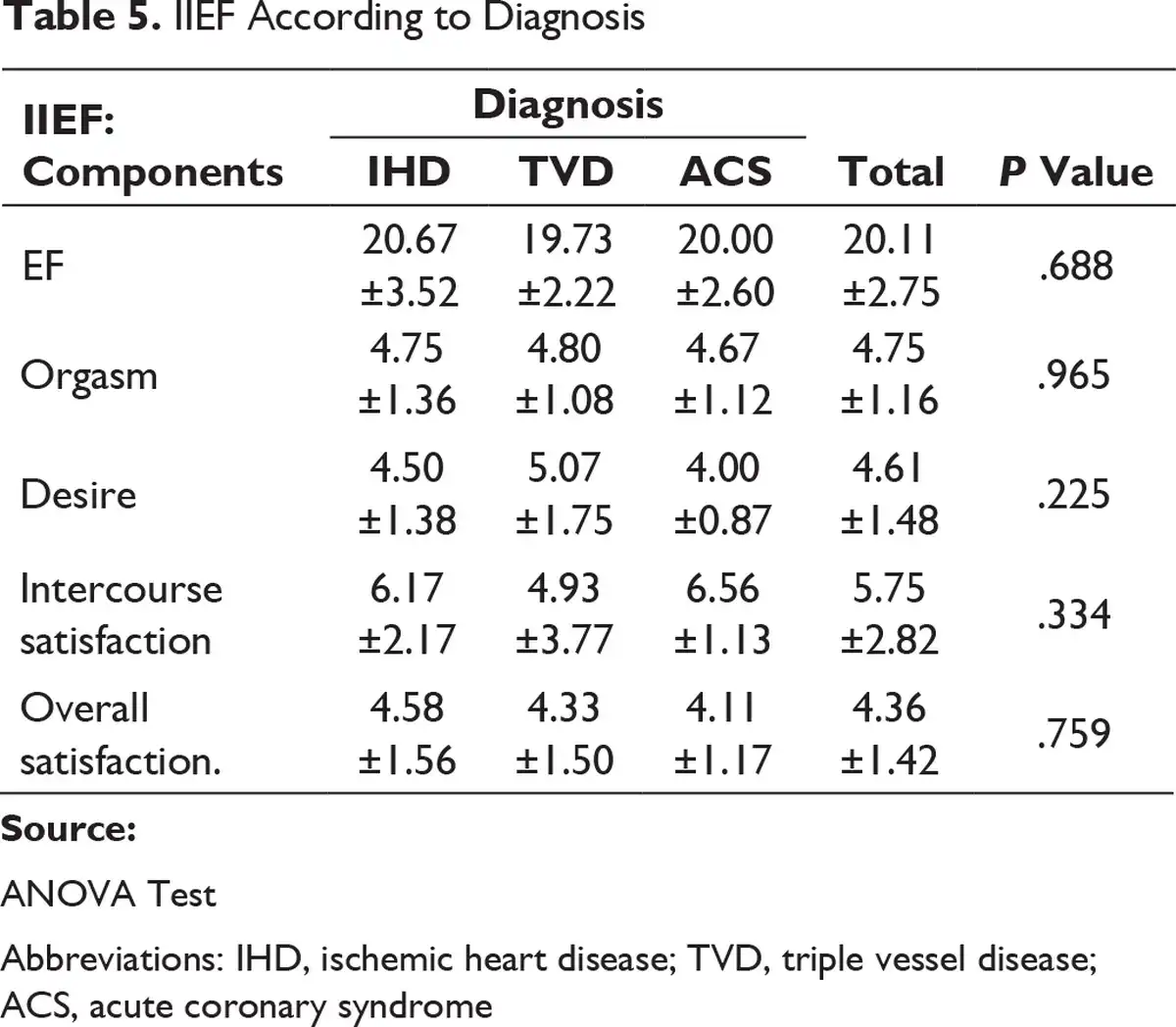
In males, 69.4% had mild ED followed by 27.8% having mild to moderate dysfunction and 2.8% had no difficulties. A total of 52.8% had moderate orgasmic dysfunction and 41.7% had mild to moderate dysfunction followed by 5.6% having mild orgasmic dysfunction. A total pf 44.4% had moderate desire problems followed by 41.7% having mild to moderate problems and 11.1% had mild problem followed by 2.8% having severe desire problems. A total of 50% had mild to moderate dysfunction in intercourse satisfaction, followed by 33.3% and 16.7% having moderate and severe dysfunction, respectively (Table 4). P value was significant for the components of desire (P < .5) and intercourse satisfaction (P < .5) (Table 5).
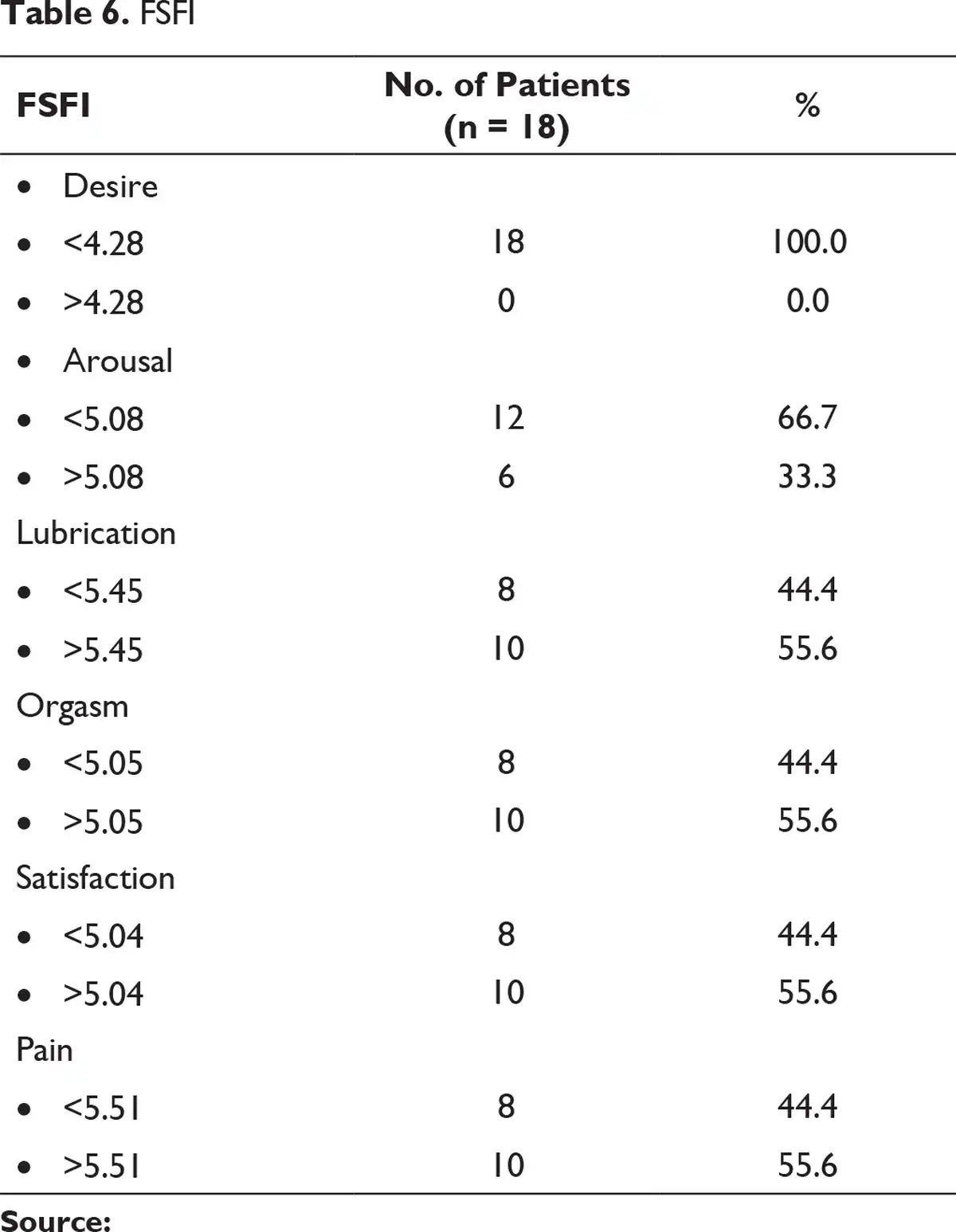
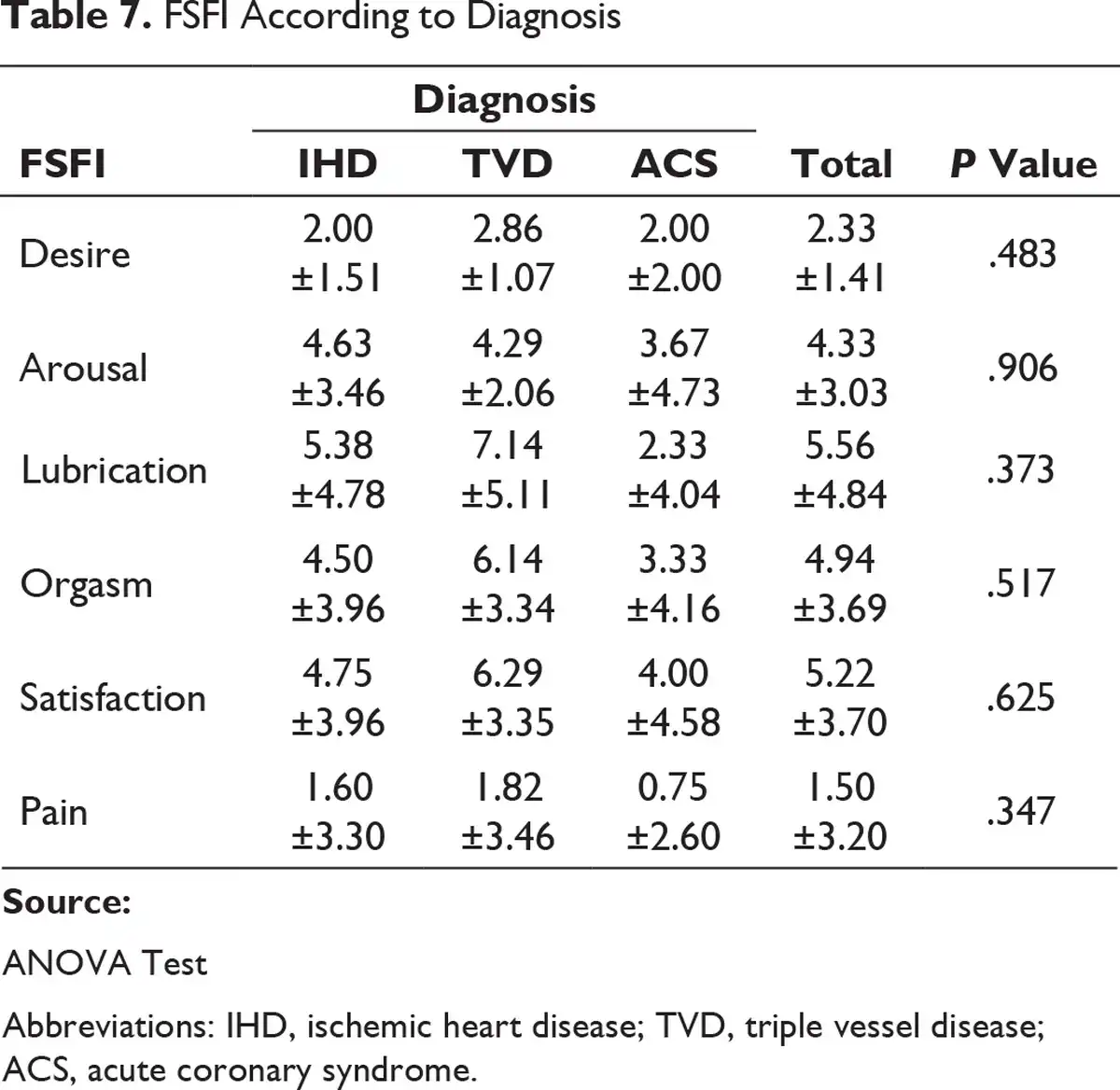
In females, 66.7% had arousal difficulties, other domains of lubrication, orgasm, satisfaction, and pain were 44.4%, and all of them had desire problems (Table 6). P value was significant for the components of lubrication and pain in relation to diagnosis (Table 7).
Discussion
Among males, 69.4% had Mild ED followed by 27.8% having mild to moderate dysfunction and 2.8% had no difficulties. A total of 52.8% had moderate dysfunction and 41.7% had mild to moderate dysfunction followed by 5.6% having mild orgasmic dysfunction. A total of 44.4% had moderate desire problems followed by 41.7% having mild to moderate problems and 11.1% had mild problem followed by 2.8% having severe desire problems. A total of 50% had mild to moderate dysfunction in intercourse satisfaction, followed by 33.3% and 16.7% having moderate and severe dysfunction, respectively. A total of 44.4% had moderate and mild to moderate dysfunction in intercourse satisfaction, followed by 5.6% of the individuals having mild and severe dysfunction. This was consistent with the study conducted by Seyed Khalil Forouzannia et al, on sex hormone levels and sexual dysfunction in men after CABG.
This shows that ED is highly prevalent in men with CVD. The relation between ED and CVD is important, but is often not considered in the same context as other common conditions, such as hypertension, dyslipidemia, IHD, or metabolic syndrome. However, vasculogenic etiology is the most implicated cause of ED in the general population. Vasculogenic ED may result from impairment of smooth muscle relaxation which may be endothelial dependent or independent (functional vascular ED), atherosclerosis leading to occlusion of penile arteries (structural vascular ED) or a combination of these two processes. Endothelial dysfunction has been established as an important process in the development of atherosclerotic CVD; therefore, it serves as a link between ED and CVD. ED preceding other manifestations of systemic atherosclerosis, such as CAD and cerebrovascular disease, may be partially explained by blood vessel size. The penile arteries measure about 1 to 2 mm in diameter, whereas the coronary arteries are 3 to 4 mm in diameter and the carotid arteries, 5 to 7 mm in diameter. Therefore, an atherosclerotic plaque should affect a penile artery earlier than a coronary or carotid artery as smaller arteries plug earlier than larger arteries. The underlying assumption of this “vessel size” theory is that slow and progressive vascular occlusion is the underlying cause of both ED and CAD, which may not always be true.
Studies have also showed that a significant proportion of men with vasculogenic ED had abnormal cardiac stress test. The chance for abnormal cardiac stress test was greater in those with corporo-venocclusive dysfunction or family history of CAD. In few cases of men presenting with ED even without a CAD history, penile doppler or cardiology referral for stress testing should be considered. The diagnosis of ED and the subsequent evaluation of underlying cardiovascular risk factors could become a powerful clinical tool in early detection of atherosclerotic disease and enhance overall health in men.
The approach to the management of these disorders are from a disease-centered perspective, often failing to incorporate the pateint’s perspective. In turn, patients frequently complain of a lack of awareness on the part of their treating doctors. From a patient-centered perspective, greater emphasis is placed on life satisfaction and quality of life as primary outcomes of treatment. Hence, a patient-centered care is relevant for both treatment and prevention of cardiac risk in men with ED, in addition to ED management in patients with or without overt CVD.
Among females, 66.7% had arousal difficulties, and other domains of lubrication, orgasm, satisfaction, and pain were 44.4% and all of them had desire problems. This is in consistence with the other studies done by Oren et al, which showed the prevalence of 76.1% sexual dysfunction.
Various other findings of this study are as follows:
There was a lack of discussion on resumption of sexual activities by the attending cardiologists.
There was hesitation in resuming sexual activity fearing precipitation of an acute cardiac event.
Among elderly, there was initial reluctance to discuss about sex and many believed that they should move towards spirituality, rather than sex, which was more common in women.
They also reported lack of adequate privacy at their dwelling places.
Many were unaware that sexual dysfunctions are related either to their medical condition or the treatment.
Hence the attending physician should discuss about the concerned issues with patients and their partners, and also try to collaborate with the Department of Psychiatry to look into the concerned issues, and identify and address the same for better outcomes.
Limitations
This is a cross-sectional study.
Longer follow-up would lead to further insights into the relation between sexual functioning and cardiac events.
A larger sample size would be helpful to determine more significant results.
Surgery itself is a stressful event, which might have led to the false positive results.
Conclusion
The findings of the study show the importance of psycho sexual issues in patients having cardiac and cardiovascular comorbidities. It is essential to incorporate enquiry, attention, and psychoeducation to all the patients attending cardiology and cardio-vascular surgery in both the out-patient and in-patient settings.
References
- Lim SS, Vos T, Flaxman AD A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2224–2260.
- Demilto L, Odle TG. Coronary artery disease. In: Longe JL, ed. The Gale Encyclopaedia of Medicine. 3rd ed. Farmington Hills, MI: Thompson Gale; 2006.
- Freedland KE, Carney RM, Davila-Roman VG, Rich MW, Skala JA, Jaffe AS. Major depression and survival in congestive heart failure. Psychosom Med. 1998;60(1):118.
- Yadava OP, Prakash A, Kundu A, Yadava M. Coronary artery bypass grafting in women: is OPCAB mandatory? Indian Heart J. 2011;63(5):425–428.
- Brister SJ, Hamdulay Z, Verma S, Maganti M, Buchanan MR. Ethnic diversity: South Asian ethnicity is associated with increased coronary artery bypass grafting mortality. J Thorac Cardiovasc Surg. 2007 Jan;133(1):150–154.
- Padmavati S. Development of cardiothoracic surgery in India. Indian J Thorac Cardiovasc Surg. 2004; 20:50–52.
- Canat L, Cicek G, Atis G, Gurbuz C, Caskurlu T. Is there a relationship between severity of coronary artery disease and severity of erectile dysfunction? Int Braz J Urol. 2013 Jul-Aug;39(4):465–473.
- Montorsi P, Montorsi F, Schulman CC. Is erectile dysfunction the “tip of the Iceberg” of a systemic vascular disorder. Eur Urol. 2003;44:352–354.
- Ronald WL, Kersten S, Meyer F Epidemiology/risk factors of sexual dysfunction. J Sex Med. 2004;1(1):35–39.
- Hultgren R, Gren BS, Derberg MSO Sexual function in women suffering from aortoiliac occlusive disease. Eur J Vasc Endovasc Surg. 1999;17(4):306–312.
- Drory Y, Kravetz S, Weingarten M. Comparison of sexual activity women and men after a first acute myocardial infarction. Am J Cardiol. 2000;85(11):1283–1287.
- Eyada M, Atwa M. Sexual function in female patients with unstable angina or non-ST-elevation myocardial infarction. J Sex Med. 2007;4(5):1373–1380.
- Kaya C, Yilmaz G, Nurkalem Z, Ilktac A, Karaman MI. Sexual function in women with coronary artery disease: a preliminary study. Int J Impot Res. 2007;19(3):326–329.
- Cook SC, Arnott LM, Nicholson LM, Cook LR, Sparks EA, Daniels CJ. Erectile dysfunction in men with congenital heart disease. Am J Cardiol. 2008;102(12):1728–1730.
- Kriston L, Guenzler C, Agvemang A, Bengel J, Berner MM. Effect sexual function on health-related quality of life mediated depressive symptoms in cardiac rehabilitation. Findings of SPARK Project in 493 patients. J Sex Med. 2010;7(6):2044–2055.
- Sathyanarayana Rao TS, Ismail S, Darshan MS, Tandon A. sexual disorders among elderly: an epidemiological study in south Indian rural population. Indian J Psychiatry. 2015; 57:236–241.
- Rosen RC, Riley A, Wagner G, Osterloh IH, Kirkpatrick J, Mishra A. The international index of erectile function (IIEF): a multidimensional scale for assessment of erectile dysfunction. Urology. 1997 Jun;49(6):822–830.
- Rosen R, Brown C, Heiman J, et al. The female sexual function index (FSFI): a multidimensional self-report instrument for the assessment of female sexual function. J Sex Marital Ther. 2000;26:191–208.
- Wiegel M, Meston C, Rosen R. The female sexual function index (FSFI): cross-validation and development of clinical cutoff scores. J Sex Marital Ther. 2005; 31:1–20.
- Forouzannia SK, Abdollahi MH, Hekmatimoghaddam S, Hassan Sayegh SA. Sex hormone levels and sexual dysfunction in men after coronary artery bypass graft. Iran J Reprod Med. 2012;10(5) 425–428.
- Salonia A, Briganti A, Deho F Pathophysiology of erectile dysfunction. Int J Androl. 2003; 26:129–136.
- Vlachopoulos C, Ioakeimidis N, Terentes-Printzios D, Stefanadis C. The triad: erectile dysfunction–endothelial dysfunction–cardiovascular disease. Curr Pharm Des. 2008; 14:3700–3714.
- Montorsi P, Ravagnani PM, Galli S The artery size hypothesis: a macrovascular link between erectile dysfunction and coronary artery disease. Am J Cardiol. 2005 Dec;96(12B):19–23.
- Mulhall J, Teloken P, Barnas J. Vasculogenic erectile dysfunction is a predictor of abnormal stress echocardiography. J Sex Med. 2009 Mar;6(3):820–825.
- Bullips KL. Sexual dysfunction and cardiovascular disease: integrative concepts and strategies. Am J Cardiol. 2005;96(12B):57–61.
- Hatzichristou D, Tsimtsiou Z. Prevention and management of cardiovascular disease and erectile dysfunction: toward a common patient-centered, care model. Am J Cardiol. 2005;96,12(2):80–84
- Oren A, Megiddo E, Banai S, Justo D. Sexual dysfunction, cardiovascular risk factors, and inflammatory biomarkers in women undergoing coronary angiography. J Women Aging. 2016;28(3):203–210.