Background
Bipolar disorder (BD) is generally a recurrent, lifelong mental health condition with a high risk of disability and excess mortality (Grande, Berk, Birmaher, & Vieta, ; Vazquez, Holtzman, Lolich, Ketter, & Baldessarini, ). The worldwide lifetime prevalence of the BD is estimated at 1% (Rowland & Marwaha, ). BD usually requires long-term medication but an estimated 40% of people are non-adherent to medication leading to relapse, functional impairment and suicidality (Gonzalez-Pinto et al., ; Lingam & Scott, ; Strakowski et al., ; Velligan et al., ). Medication non-adherence increases the probability of hospitalisation by at least five times (Scott & Pope, ).
Efforts to improve medication adherence have had marginal effects (Easthall, Taylor, & Bhattacharya, ; Nieuwlaat et al., ). This may be due to limited understanding of the modifiable determinants of medication adherence and existing support focussing on a narrow range of adherence determinants. We define modifiable determinants as ‘any determinants (barriers or facilitators) of medication adherence that can be modified by the patient, carer, or the prescriber within a short timeframe (days or weeks) to improve adherence’. We define a barrier as ‘a circumstance that prevents the patient from taking their medication as prescribed’, whereas a facilitator is ‘a circumstance that makes the process easy or easier’ (Oxford English dictionary online: Oxford university press, ). Some evidence syntheses report determinants of adherence to mental health treatment but they do not clearly distinguish between those that are modifiable, such as knowledge regarding how to take medication and non-modifiable such as age and gender. Such distinction is vital to allow adherence interventions to target modifiable determinants.
Furthermore, any differences between the perspective of clinicians and patients on determinants of medication adherence require exploration. Clinicians are the treatment experts but patients are the experts of their lived experience. Their goals, priorities and knowledge of the situation may differ. Thus, clinicians and patients may see the determinants of medication adherence differently (Devine, Edwards, & Feldman, ; Velligan et al., ). Exploring such differences will help design adherence support based on the patient's needs.
A recent systematic review by Garcia et al. provides an overview of barriers to medication adherence in BD and schizophrenia (Garcia et al., ). However, the study limited on determinants of adherence to antipsychotics (one group of medication to manage BD). Other common medications for BD are known as mood stabilisers which includes lithium. The omission of adherence determinants to lithium and other mood stabilisers is significant since lithium is recognised as the first-line gold standard long-term therapy in BD [Grunze et al., ; National Institute of Health and Care Excellence (NICE), ]. It is also noteworthy that the challenges to adhere to lithium may be different as lithium is a narrow therapeutic index drug and thus require a regular blood test, some dietary restrictions and has significant interactions with other medications [National Institute of Health and Care Excellence (NICE), ]. Furthermore, the review does not delineate modifiable from non-modifiable determinants which lack specific behaviour change techniques (BCTs) (Michie, Johnston, Francis, & Hardeman, ).
Additionally, the lack of behavioural theory underpinning the evidence synthesis in medication adherence in BD is evident. Thus, a systematic review of modifiable determinants of all treatment option in BD underpinned by theoretical framework is needed. Further details regarding the rationale for this systematic review are provided in the published protocol (Prajapati et al., ).
This systematic review aimed to identify modifiable determinants of medication adherence in BD reported in the literature and map them to the theoretical domains framework (TDF).
This study is a part of the Collaborative Medication Adherence in Bipolar disorder (C-MAB) project funded by Health Education England/National Institute for Health Research UK. The C-MAB project aims to develop a medication adherence tool for people with BD. The project advisory board includes stakeholders, patients, carers, clinicians, health psychologist and experts in behavioural medicine.
Method
The study was registered with PROSPERO, registration number: CRD42018096306.
The protocol with detailed methods for this systematic review is published elsewhere (Prajapati et al., ), and a summary of the methods is provided below.
We searched CINAHL, Cochrane Library, Embase, LILACS, Medline, PsychINFO and PubMed from database inception to October 2018 using the search terms ‘Treatment Adherence and Compliance’, ‘Bipolar Disorder’ and ‘Psychotropic Drugs’. We updated the search in February 2020. The detailed search strategy is available in online Supplementary file.
We included primary, qualitative and quantitative studies published in the English language and studies explicitly reporting modifiable determinants of medication adherence in BD in adults. We excluded reviews, intervention studies to improve adherence, case reports, clinical guidelines or general disease management articles, studies involving short-term treatment of acute agitation or treatment other than medication such as psychotherapy.
Two reviewers (AP, DB, FS, GM, JW and SS) independently screened the study abstracts and full-texts and carried out the quality assessment. Disagreements were resolved through discussion and referral to a third reviewer for arbitration if necessary. A range of quality assessment tools (Center for Evidence Based Management, ; Critical Appraisal Skills Programme, ; National Institute of Health, ) was used according to the study designs (Frambach, van der Vleuten, & Durning, ).
We used Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Moher, Liberati, Tetzlaff, Altman, & The PRISMA Group, ) checklist for data extraction and reporting. The completed PRISMA checklist is available in online Supplementary file 2.
Underpinning theoretical framework
We used framework analysis with the TDF as an a priori framework, to map modifiable determinants of medication adherence to their relevant TDF domain. The use of a theoretical framework provides a broad lens through which to capture the literature identified modifiable determinants. The TDF is a comprehensive framework capturing 33 theories and 84 theoretical constructs related to behaviour change (Atkins et al., ). Atkins et al. report the definition of each TDF domain and construct within each domain (Atkins et al., ). TDF was developed as a consensus framework by experts in health service research and behaviour science (Michie et al., ). The TDF offers the additional advantage that each of its 14 domains is coupled with BCTs (Michie et al., ). Thus, mapping modifiable determinants of adherence to the TDF offers a significant utility for intervention development.
Two independent reviewers (AP, AD, DB and SS), with experience in using the TDF, extracted modifiable determinants and coded them to the TDF domains using Nvivo 12 (QSR International Pty Ltd, ). For example, the extracted text ‘lack of awareness that medication needed to be taken regularly led to non-adherence’ in the study was coded to the TDF domain ‘Knowledge’. In addition to the 14 TDF domains, we also created another domain called ‘Others’ for any modifiable determinant not suitable to map to those 14 domains. Agreement between two reviewers in mapping modifiable determinants to the same TDF domain was calculated in SPSS version 25 using Cohen's kappa.
We grouped the modifiable determinants into overarching themes (Gale, Heath, Cameron, Rashid, & Redwood, ). We also coded whether the modifiable determinants were barriers or facilitators and whether it was reported by patients, clinicians, carers or any other third parties.
Results
From the 2517 studies retrieved, we included 57, comprising 32 894 patients and clinicians. Figure 1 provides the screening process, number of retrieved studies, number of studies included and excluded during title screening, abstract screening and full text screening as well as the reasons for exclusion. The primary reasons for exclusion at full-text screening were failure to report modifiable determinants or reporting an intervention to address adherence.
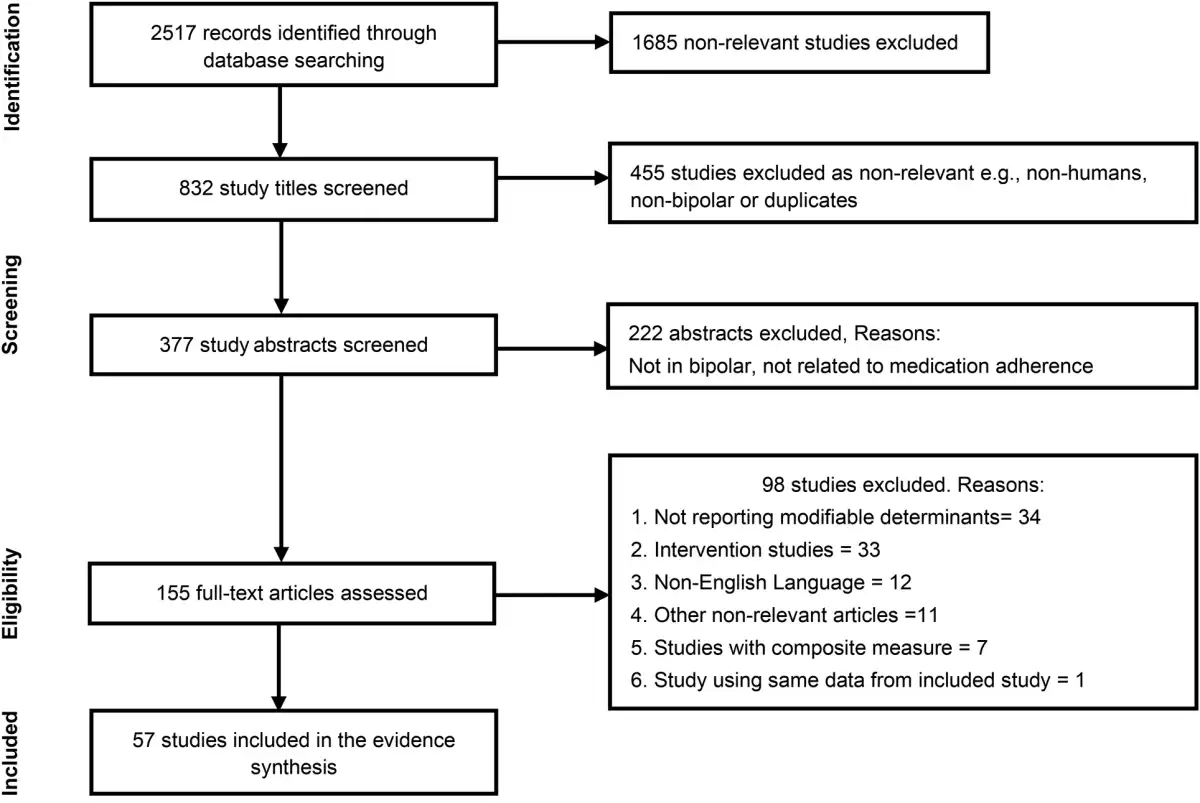
Fig. 1
PRISMA flow diagram.
PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study characteristics
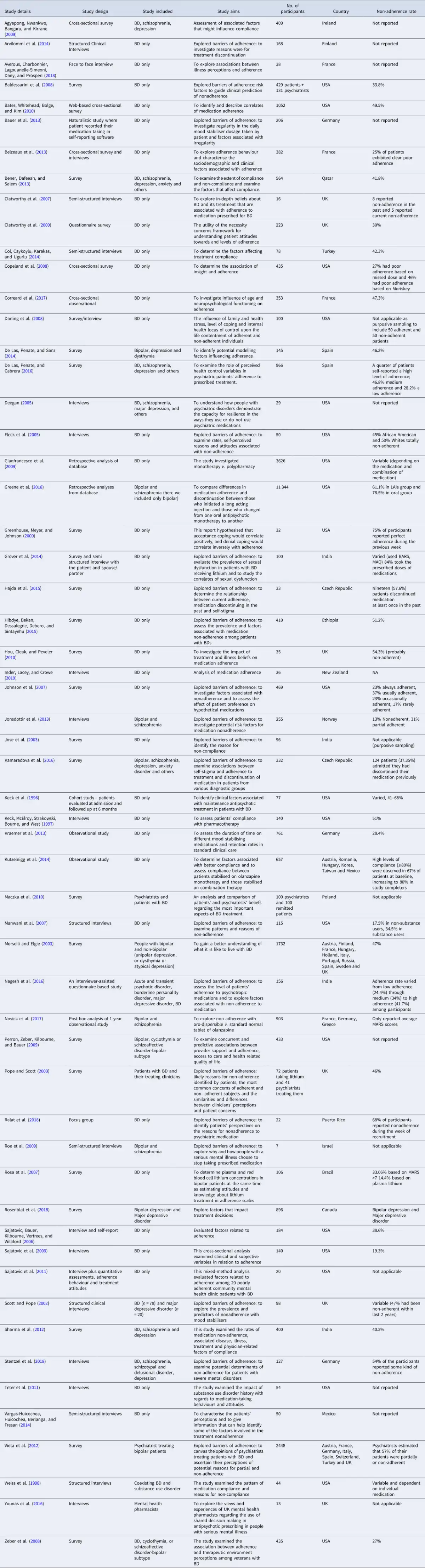
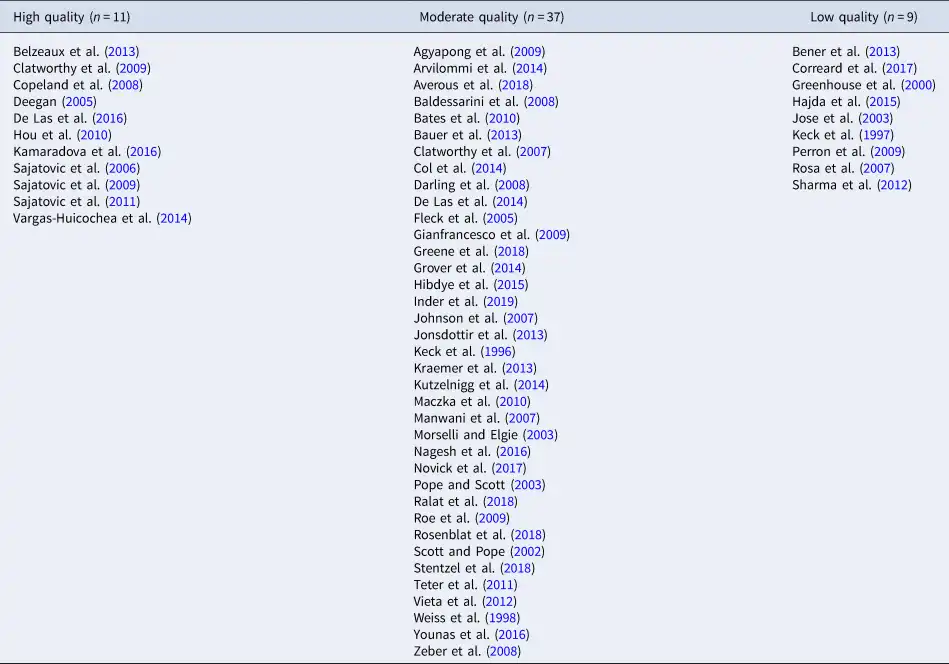
Summary characteristics such as study design, participant details and, country in which the included study was conducted are presented in Table 1. Fifty studies explored determinants from the perspective of patients and two (Vieta et al., ; Younas, Bradley, Holmes, Sud, & Maidment, ) from clinicians' perspective. Three studies included both patient and clinician perspectives (Baldessarini, Perry, & Pike, ; Maczka, Siwek, Skalski, Grabski, & Dudek, ; Pope & Scott, ). Further two studies were from the researcher's perspective (Gianfrancesco, Sajatovic, Tafesse, & Wang, ; Greene et al., ). However, none of the studies included carers. Most of the included studies collected data via surveys or interviews. The majority (79%) of the studies were conducted in the USA and Europe. A majority of the studies (64%) were focused purely on BD. Of the 57 included studies, 33% (Arvilommi et al., ; Baldessarini et al., ; Bauer et al., ; Fleck, Corey, Strakowski, & Keck, ; Grover, Ghosh, Sarkar, Chakrabarti, & Avasthi, ; Hajda et al., ; Johnson et al., ; Jonsdottir et al., ; Jose, Bhaduri, & Mathew, ; Manwani et al., ; Nagesh, Kishore, & Raveesh, ; Pope & Scott, ; Ralat, Depp, & Bernal, ; Roe, Goldblatt, Baloush-Klienman, Swarbrick, & Davidson, ; Scott & Pope, ; Stentzel et al., ; Vieta et al., ) explicitly focused on exploring barriers to adherence. Table 2 describes the quality of the included studies. The majority (65%) of the studies was of moderate quality, 19% were of high quality and 16% were of low quality.
Reported modifiable determinants of medication adherence
We extracted 290 modifiable determinants, which were grouped into 33 themes and mapped to 11 TDF domains. Inter-rater reliability for mapping the modifiable determinants to the TDF domains was 76% (Cohen's kappa 0.71), indicating substantial agreement between the reviewers (Landis & Koch, ). Cohen's kappa was calculated using SPSS 25.0 (IBM Corporation, ). Examples of the modifiable determinants, themes of determinants and TDF domains to which they were mapped are reported in Table 3.
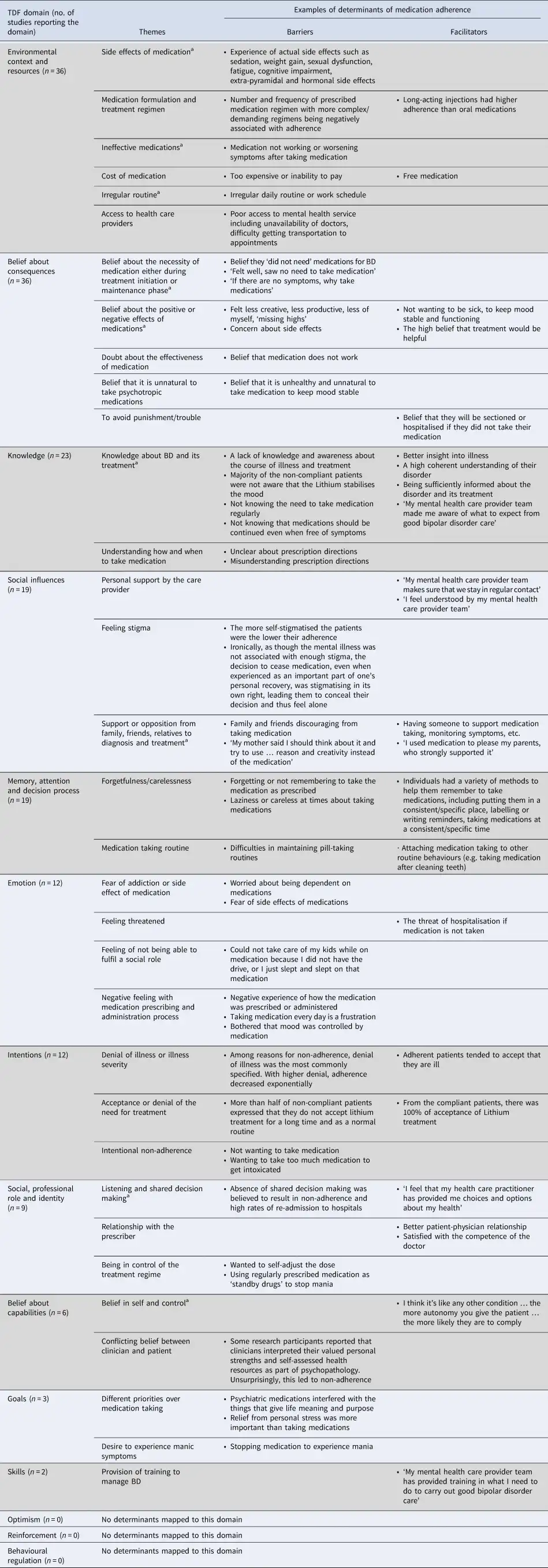
Some facilitators were reported as the opposite of barriers. For example, ‘cost of medication’ was identified as a barrier in the ‘Environmental context and resources’ domain, for which ‘medication being free of charge’ represented the corresponding facilitator. In other cases, facilitators were occasionally worded as BCTs. For example, forgetfulness represented a barrier in the ‘memory, attention, and decision processes’ domain, for which the corresponding facilitators were reminders and formulating routines; these were classified in the BCT category of ‘prompts and cues’ which may successfully modify behaviour by addressing determinants in this TDF domain (Johnston et al., ).
The TDF domains represented in the greatest number of studies were ‘Environmental context and resources’ (63% of studies) and ‘Beliefs about consequences’ (63% of studies). Experience of side effects (49% of studies) and the nature of the medication, e.g. tablet, injection and dose frequency (22% of studies) were the main determinants mapped to the former; acting as barriers when unacceptable and facilitators when acceptable to patients. Beliefs about the likely positive/negative outcomes arising from adhering (36% of studies) and a belief that the medication is not needed (25% of studies) were the main determinants mapped to the latter.
Other TDF domains (and corresponding themes of determinants) reported in 20% or more studies, among all studies, were ‘Knowledge’ (whether the patient had sufficient knowledge about BD or its treatment); ‘Social influences’ (support or opposition from family, friends, relatives, clinicians regarding adherence); ‘Emotion’ (fear of addiction to or side effect from medication); ‘Memory, attention, and decision process’ (forgetfulness/carelessness with medication taking) and ‘Intentions’ (denial of illness or need for treatment).
Modifiable determinants were most frequently reported in the context of barriers rather than facilitators. However, unlike most other TDF domains, for ‘social influences’, facilitators and barriers were reported with similar frequency. This trend was also observed for ‘Social/Professional Role and identity’. Modifiable determinants related to ‘Goals’ and ‘Skills’ were infrequently reported. No determinants were mapped to the TDF domains of ‘Optimism’, ‘Reinforcement’ and ‘Behavioural regulation’.
Determinants from the perspectives of patients and clinicians
Figure 2 illustrates the TDF domains reported in patient studies compared to clinician studies. ‘Beliefs about consequences’ and ‘Environmental context and resources’ were the two most frequently reported TDF domains in both patient studies as well as clinicians studies. There were, however, noticeable differences in the range and nature of determinants reported by patients relative to clinicians. Determinants reported by clinicians were mapped to only six TDF domains compared to 11 TDF domains covered by patient studies. Only patient studies reported determinants which were mapped to the TDF domains ‘Intention’, ‘Memory, attention and decision process’ and ‘Emotion’. These domains included determinants such as denial of the illness or need for treatment, forgetfulness/carelessness and fear of addiction to or side effect of medication respectively (see Table 3 for more details).
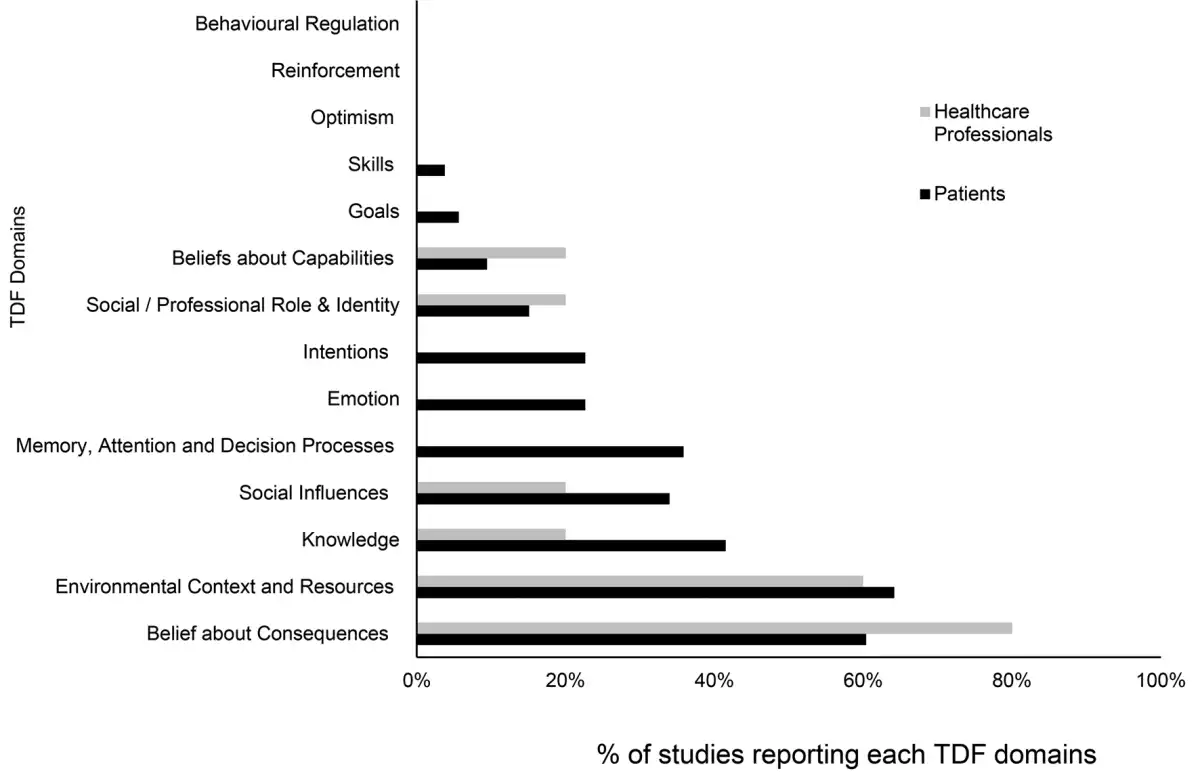
Fig. 2
Comparison of TDF domains reported by patients and clinicians. No. of patients only studies = 50; no. of clinicians only studies = 2; no. of studies including patients and clinicians = 3. Two studies exploring researchers' perspectives were not included in this graph.
Furthermore, ‘Goals’ and ‘Skills’ domains were reported in patient studies, albeit infrequently. An example of determinants in these two domains includes different priorities over medication taking and provision of training to manage BD, as shown in Table 3.
Clinicians reported modifiable determinants of adherence themed around lack of knowledge about medication, shared decision making, belief in self and perceived control, belief that medication is not needed, belief about positive or negative effects of medication, side effects, ineffective medication and irregular routine.
Two studies reported determinants from the researcher perspective (Gianfrancesco et al., ; Greene et al., ) namely medication formulations (such as tablets and injections) and the number of medications, both of which were mapped to ‘Environmental context and resources’ domain.
Discussion
Synthesis of the literature through the theoretical lens of the TDF has enabled us to identify that negative emotions evoked by medication taking and intentional non-adherence make a notable contribution to non-adherent behaviour. In contrast to the focus of existing interventions on practical barriers to adherence (MacDonald, ; Torres-Robles et al., ), clinicians should additionally address negative emotions and lack of intentions.
In common with previous evidence syntheses, modifiable determinants were primarily barriers to adherence (Garcia et al., ; Velligan et al., ) with few reported facilitators. This may be an artefact of the included studies focussing on the challenges experienced by patients, rather than seeking to explore potential solutions. This hypothesis is supported by a third of the included studies explicitly seeking only barriers to medication adherence. For the few studies exploring facilitators, determinants that are not the opposite of barriers, such as wanting to keep the mood stable and not wanting to be hospitalised, have also been reported (Clatworthy, Parham, Horne, Bowskill, & Rank, ; Darling, Olmstead, Lund, & Fairclough, ). A strength of the present review is that we did not restrict the search to only adherence barriers; thus, we have identified a gap in the literature.
Current adherence interventions in BD focus mostly on education regarding medication and BD, cognitive therapy to address negative attitudes and beliefs, family therapy to encourage social support and technology to address forgetfulness (MacDonald, ; Torres-Robles et al., ). Furthermore, adherence support in the UK focusses on shared decision making regarding the choice of medication, side effects profile of medication, cost of medication and exploring patients beliefs [Care Quality Commission (CQC), ; National Institute of Healthand Care Excellence (NICE), ]. However, in this study, we found a broad range of other modifiable determinants that may be affecting medication adherence. This study provides clinicians with a comprehensive list of modifiable determinants of medication adherence, some of which are underappreciated by clinicians and unaddressed by existing adherence interventions.
Advantages of mapping modifiable determinants to the TDF
Mapping determinants to the TDF allows them to be linked to BCTs. Thus, this study provides a foundation for developing a complex adherence intervention tailored to patients' needs based on their predominant determinants of adherence. The most frequently reported TDF domains of ‘Beliefs about consequences’ and ‘Environmental context and resources’ indicate that working with the patient's belief system, medication acceptability and tolerability are vital to support medication adherence. However, other modifiable determinants, particularly in ‘Intentions’, ‘Memory, attention and decision process’ and ‘Emotion’ domains, presented in this study may be equally or more relevant to individual patients. Thus, identifying the modifiable determinants most pertinent to an individual patient is critical to providing patient-centred adherence support.
The most frequently reported domain ‘Environmental context and resources’ was primarily related to medication characteristics such as side effects, treatment regime, medication effectiveness or cost of medication, etc. This finding accords with previous studies (Garcia et al., ; Kikkert et al., ; Salzmann-Erikson & Sjodin, ; Velligan et al., ). Side effects were represented in the domains of both ‘Environmental context and resources’ and ‘Beliefs about consequences’. This was because patients reported non-adherence arising from both experiencing side effects and being concerned that side effects may result from taking the medication. Each requires a different BCT, for example, the former may be better addressed by ‘restructuring the physical environment,’ e.g. by changing medication with a lower propensity of a particular side effect that the patient is experiencing. In contrast, the latter aligns with BCTs such as ‘pros and cons,’ e.g. discussing the risk and benefit of taking and not taking the medication (The UCL Centre for Behaviour Change, ).
The dominance of ‘Beliefs about consequences’ on medication adherence in this review is supported by other studies using the TDF (Crayton et al., ; Easthall et al., ). Belief about the necessity or concerns of medication were frequently reported determinants of adherence within this domain. As often reported in clinical practice, many people stop taking their medication once they feel better believing they no longer need them. On the contrary, some people believe they do not need medication at the start of the treatment and thus do not initiate them. Therefore, BCTs such as ‘pros and cons’ may play a vital role in medication adherence (The UCL Centre for Behaviour Change, ).
The absence of determinants mapped to the TDF domains ‘Optimism’, ‘Reinforcement’ and ‘Behavioural regulation’ does not necessarily mean that these three domains are unimportant to medication adherence in BD. Previous studies may not have explored these specific domains. Some adherence intervention studies suggest ‘Reinforcement’ using financial incentives may improve adherence (Priebe, Bremner, Lauber, Henderson, & Burns, ). Similarly, optimism, as measured by the revised Life Orientation Test (Herzberg, Glaesmer, & Hoyer, ), was reported to lead to improved adherence in acute coronary syndrome (Millstein et al., ). Revised Life Orientation Test includes statements such as ‘Overall, I expect more good things happen to me than bad’, ‘In uncertain times, I usually expect the best’ (Herzberg et al., ). However, these may not be modifiable. Future study should explicitly investigate the extent to which these unrepresented domains are relevant to non-adherence in this population and whether they are modifiable in the context of medication adherence.
Although there was a significant overlap between determinants reported by clinicians and patients, there were also notable distinctions. These distinctions may explain the limited progress made by clinicians in identifying and addressing non-adherence (Hartung et al., ; Nieuwlaat et al., ). However, these distinctions may also have arisen due to the small number of studies exploring the clinician's perspective.
Clinician reported determinants mapped to less than half of the TDF domains, suggesting that clinicians may not be aware of the broad range of determinants affecting medication adherence or studies were not designed to elicit this information from clinicians. The influence of negative emotion evoked by taking medication and intentional non-adherence was the most notable omission from clinicians' perspectives. This incomplete picture may result in adherence support poorly reflecting patients' needs (Brown et al., ). This is evident from current adherence support being focused on a very limited number of determinants (MacDonald, ; National Institute of Healthand Care Excellence (NICE), ; Thompson, Kulkarni, & Sergejew, ; Torres-Robles et al. ).
Strengths and limitations
This study offers three novel aspects in the field of medication adherence research in BD. Firstly, the study focuses on potential adherence intervention targets by reporting only modifiable determinants. Secondly, as the application of theory is a core requirement for developing and implementing complex interventions, our use of a theoretical framework provides the foundations for developing future medication adherence interventions and their implementation. Finally, the comprehensive nature of a theoretical framework rather than an individual theory has enabled us to identify gaps in the literature.
Using the TDF as an a priori framework to organise modifiable determinants is a deductive approach. However, we did not constrain extraction of the determinants and mapping them to only the TDF domains as any determinants not aligned to the TDF would have been captured in the ‘Others’ category. The lack of detailed description of the determinants in some studies risked mapping them to incorrect TDF domains. For example, some studies described ‘hassle to acquire medication’ as a determinant of adherence. It could mean the patient has difficulty obtaining medication due to not knowing how to order their prescription or difficulty remembering to order a prescription or lack of transport/money/time to order prescription. Each interpretation would be mapped to a different TDF domain. Further qualitative study with patients will facilitate these further refinements in mapping.
We presented the modifiable determinants of adherence identified from a wide range of study designs. We recognise that the medium via which data are collected can influence the range of determinants captured. For example, interviews may elicit a greater range of determinants that are personal to the individual v. a structured survey of potentially relevant determinants (Lagard, Keegan, & Ward, ). This non-restrictive approach has contributed to identifying a list of modifiable determinants as comprehensively as possible which was one of the goals of this study.
Implications for practice
We provide theory and evidence-based modifiable determinants that influence a patient's ability to adhere to their prescribed medication. All these determinants should, therefore, be considered and potentially discussed with patients when initiating treatment and at every review. Currently, clinicians may not be providing adherence support tailored to patients' wide-ranging needs.
Implications for research
The application of a theoretical framework to the systematic review has enabled us to identify gaps in the literature where researchers have not sought to investigate the relevance of facilitators of adherence. Further research to explicitly capture the facilitators of adherence may help design future adherence interventions. The existing literature mostly represents the patient voice; absence of the carer voice is a notable gap given their role in supporting medication adherence in people with mental health problems (Deane, McAlpine, Byrne, Davis, & Mortimer, ). Future research exploring carers' views on modifiable determinants of medication adherence in BD is, therefore, needed.
Acknowledgements
We would like to thank members of the Collaborative Medication Adherence in Bipolar disorder (C-MAB) Research Advisory Board members for their support. We are also grateful to colleagues from NSFT and UEA libraries for help with the literature search and sourcing articles.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0033291721001446
Author contributions
All authors contributed to the development of the protocol for this systematic review. AP led the literature search. AP, DB, GM, JW and SS screened the abstract and full text. AP, GM, JW and FS extracted data. AP, GM and FS quality assessed included studies. AP, AD, DB and SS extracted modifiable determinants and mapped to the TDF. AP and DB led manuscript preparation. All authors read and approved the final manuscript.
Financial support
Asta Ratna Prajapati is funded by Health Education England (HEE)/National Institute for Health Research (NIHR) (Clinical Doctoral Research Fellowship) (NIHR reference number: ICA-CDRF-2017-03-054) for this research project. This paper presents independent research funded by the National Institute for Health Research (NIHR). The views expressed are those of the author(s) and not necessarily those of the NHS, the HEE/NIHR, or the Department of Health and Social Care.
Conflict of interest
None.
References
- Agyapong V. I. O., Nwankwo V., Bangaru R., & Kirrane R. (2009). Sources of patients' knowledge of the adverse effects of psychotropic medication and the perceived influence of adverse effects on compliance among service users attending community mental health services. Journal of Clinical Psychopharmacology, 29(6), 565–570.
- Arvilommi P., Suominen K., Mantere O., Valtonen H., Isometsa E., & Leppamaki S. (2014). Predictors of adherence to psychopharmacological and psychosocial treatment in bipolar I or II disorders – An 18-month prospective study. Journal of Affective Disorders, 155(1), 110–117.
- Atkins L., Francis J., Islam R., O'Connor D., Patey A., Ivers N., … Michie S. (2017). A guide to using the theoretical domains framework of behaviour change to investigate implementation problems. Implementation Science, 12, 77–95. doi:
- Averous P., Charbonnier E., Lagouanelle-Simeoni M. C., Dany L., & Prosperi A. (2018). Illness perceptions and adherence in bipolar disorder: An exploratory study. Comprehensive Psychiatry, 80, 109–115.
- Baldessarini R. J., Perry R., & Pike J. (2008). Factors associated with treatment nonadherence among US bipolar disorder patients. Human Psychopharmacology, 23(2), 95–105.
- Bates J. A., Whitehead R., Bolge S. C., & Kim E. (2010). Correlates of medication adherence among patients with bipolar disorder: Results of the bipolar evaluation of satisfaction and tolerability (BEST) study: A nationwide cross-sectional study. Primary Care Companion to the Journal of Clinical Psychiatry, 12(5), E1–E8. doi: .
- Bauer M., Glenn T., Alda M., Sagduyu K., Marsh W., Grof P., … Whybrow P. C. (2013). Regularity in daily mood stabilizer dosage taken by patients with bipolar disorder. Pharmacopsychiatry, 46(5), 163–168.
- Belzeaux R., Correard N., Azorin J.-M., Etain B., Loftus J., Bellivier F., … Boyer L. (2013). Depressive residual symptoms are associated with lower adherence to medication in bipolar patients without substance use disorder: Results from the FACE-BD cohort. Journal of Affective Disorders, 151(3), 1009–1015.
- Bener A., Dafeeah E. E., & Salem M. O. (2013). A study of reasons of non-compliance of psychiatric treatment and patients' attitudes towards illness and treatment in Qatar. Issues in Mental Health Nursing, 34(4), 273–280.
- Brown T., Twigg M., Taylor N., Easthall C., Hartt J., Budd T., … Bhattacharya D. (2017). Final report for the IMAB-Q study: Validation and feasibility testing of a novel questionnaire to identify barriers to medication adherence. London, UK. Retrieved May 5, 2020, from https://pharmacyresearchuk.org/wp-content/uploads/2017/01/IMAB-Q-validation-and-feasibility-testing-full-report.pdf.
- Care Quality Commission (CQC). (2018). NHS patient survey programme: 2018 community mental health survey, Statistical release, 30-34. Retrieved May 5, 2020, from https://www.cqc.org.uk/sites/default/files/20181122_cmh18_statisticalrelease.pdf.
- Center for Evidence Based Management. (2014). Critical Appraisal Checklists for a Qualitative Study. Retrieved May 10, 2020, from https://www.cebma.org.
- Clatworthy J., Bowskill R., Parham R., Rank T., Scott J., & Horne R. (2009). Understanding medication non-adherence in bipolar disorders using a necessity-concerns framework. Journal of Affective Disorders, 116(1), 51–55.
- Clatworthy J., Parham R., Horne R., Bowskill R., & Rank T. (2007). Adherence to medication in bipolar disorder: A qualitative study exploring the role of patients' beliefs about the condition and its treatment. Bipolar Disorders, 9(6), 656–664.
- Col S. E., Caykoylu A., Karakas U. G., & Ugurlu M. (2014). Factors affecting treatment compliance in patients with bipolar I disorder during prophylaxis: A study from Turkey. General Hospital Psychiatry, 36(2), 208–213.
- Copeland L. A., Zeber J. E., Salloum I. M., Pincus H. A., Fine M. J., & Kilbourne A. M. (2008). Treatment adherence and illness insight in veterans with bipolar disorder. The Journal of Nervous and Mental Disease, 196(1), 16–21.
- Correard N., Consoloni J.-L., Azorin J.-M., Belzeaux R., Raust A., Etain B., … Beetz E. (2017). Neuropsychological functioning, age, and medication adherence in bipolar disorder. PLoS ONE, 12(9), e0184313.
- Crayton E., Fahey M., Ashworth M., Besser S. J., Weinman J., & Wright A. J. (2017). Psychological determinants of medication adherence in stroke survivors: A systematic review of observational studies. Annals of Behavioral Medicine: A Publication of the Society of Behavioral Medicine, 51(6), 833–845. doi:
- Critical Appraisal Skills Programme (CASP). (2018). 10 questions to help you make sense of qualitative research. CASP qual checkl. Oxford: UK. Retrieved May 5, 2020, from https://casp-uk.net/.
- Darling C. A., Olmstead S. B., Lund V. E., & Fairclough J. F. (2008). Bipolar disorder: Medication adherence and life contentment. Archives of Psychiatric Nursing, 22(3), 113–126.
- Deane F. P., McAlpine E., Byrne M. K., Davis E. L., & Mortimer C. (2018). Are carer attitudes toward medications related to self-reported medication adherence amongst people with mental illness? Psychiatry Research, 260, 158–163. doi:
- Deegan P. E. (2005). The importance of personal medicine: A qualitative study of resilience in people with psychiatric disabilities. Scandinavian Journal of Public Health, 33, 29–35.
- De Las C. C., Penate W., & Cabrera C. (2016). Perceived health control: A promising step forward in our understanding of treatment adherence in psychiatric care. Journal of Clinical Psychiatry, 77(10), e1233-e1239. doi:
- De Las C. C., Penate W., & Sanz E. J. (2014). Risk factors for non-adherence to antidepressant treatment in patients with mood disorders. European Journal of Clinical Pharmacology, 70(1), 89–98.
- Devine F., Edwards T., & Feldman S. R. (2018). Barriers to treatment: Describing them from a different perspective. Patient Preference and Adherence, 12, 129–133. doi:
- Easthall C., Taylor N., & Bhattacharya D. (2019). Barriers to medication adherence in patients prescribed medicines for the prevention of cardiovascular disease: A conceptual framework. The International Journal of Pharmacy Practice, 27(3), 223–231. doi:
- Fleck D.E., Corey K.B., Strakowski S.M., & Keck Jr. P.E. (2005). Factors associated with medication adherence in African American and white patients with bipolar disorder. Journal of Clinical Psychiatry, 66(5), 646–652.
- Frambach J. M., van der Vleuten C. P., & Durning S. J. (2013). AM last page. Quality criteria in qualitative and quantitative research. Academic Medicine: Journal of the Association of American Medical Colleges, 88(4), 552. doi:
- Gale N. K., Heath G., Cameron E., Rashid S., & Redwood S. (2013). Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Medical Research Methodology, 13, 117–2288-13-117. doi: .
- Garcia S., Martinez-Cengotitabengoa M., Lopez-Zurbano S., Zorrilla I., Lopez P., Vieta E., & Gonzalez-Pinto A. (2016). Adherence to antipsychotic medication in bipolar disorder and schizophrenic patients: A systematic review. Journal of Clinical Psychopharmacology, 36(4), 355–371. doi:
- Gianfrancesco F. D., Sajatovic M., Tafesse E., & Wang R. H. (2009). Association between antipsychotic combination therapy and treatment adherence among individuals with bipolar disorder. Annals of Clinical Psychiatry, 21(1), 3–16.
- Gonzalez-Pinto A., Mosquera F., Alonso M., Lopez P., Ramirez F., Vieta E., & Baldessarini R. J. (2006). Suicidal risk in bipolar I disorder patients and adherence to long-term lithium treatment. Bipolar Disorders, 8(5), 618–624.
- Grande I., Berk M., Birmaher B., & Vieta E. (2016). Bipolar disorder. Lancet (London, England), 387(10027), 1561–1572. doi:
- Greene M., Yan T., Chang E., Broder M. S., Hartry A., & Touya M. (2018). Medication adherence and discontinuation of long-acting injectable versus oral antipsychotics in patients with schizophrenia or bipolar disorder. Journal of Medical Economics, 21(2), 127–134.
- Greenhouse W. J., Meyer B., & Johnson S. L. (2000). Coping and medication adherence in bipolar disorder. Journal of Affective Disorders, 59(3), 237–241.
- Grover S., Ghosh A., Sarkar S., Chakrabarti S., & Avasthi A. (2014). Sexual dysfunction in clinically stable patients with bipolar disorder receiving lithium. Journal of Clinical Psychopharmacology, 34(4), 475–482.
- Grunze H., Vieta E., Goodwin G. M., Bowden C., Licht R. W., Moller H. J., … WFSBP Task Force on Treatment Guidelines for Bipolar Disorders. (2013). The world federation of societies of biological psychiatry (WFSBP) guidelines for the biological treatment of bipolar disorders: Update 2012 on the long-term treatment of bipolar disorder. The World Journal of Biological Psychiatry, 14(3), 154–219. doi: .
- Hajda M., Kamaradova D., Latalova K., Prasko J., Ociskova M., Mainerova B., … Tichackova A. (2015). Self-stigma, treatment adherence, and medication discontinuation in patients with bipolar disorders in remission – A cross sectional study. Activitas Nervosa Superior Rediviva, 57(1), 6–11.
- Hartung D., Low A., Jindai K., Mansoor D., Judge M., Mendelson A., … Kondo K. (2017). Interventions to improve pharmacological adherence among adults with psychotic spectrum disorders and bipolar disorder: A systematic review. Psychosomatics, 58(2), 101–112. doi:
- Herzberg P. Y., Glaesmer H., & Hoyer J. (2006). Separating optimism and pessimism: A robust psychometric analysis of the revised life orientation test (LOT-R). Psychological Assessment, 18(4), 433–438. doi:
- Hibdye G., Bekan L., Dessalegne Y., Debero N., & Sintayehu M. (2015). Prevalence of drug non adherence and associated factors among patients with bipolar disorder at outpatient unit of Amanuel Hospital, Addis Ababa, Ethiopia, 2013. African Journal of Psychiatry (South Africa), 18, 1–7.
- Hou R., Cleak V., & Peveler R. (2010). Do treatment and illness beliefs influence adherence to medication in patients with bipolar affective disorder? A preliminary cross-sectional study. European Psychiatry, 25(4), 216–219.
- IBM Corp. (2017). IBM SPSS statistics for windows. Armonk, NY: IBM Corp.
- Inder M., Lacey C., & Crowe M. (2019). Participation in decision-making about medication: A qualitative analysis of medication adherence. International Journal of Mental Health Nursing, 28(1), 181–189. doi:
- Johnson F. R., Ozdemir S., Manjunath R., Hauber A. B., Burch S. P., & Thompson T. R. (2007). Factors that affect adherence to bipolar disorder treatments: A stated-preference approach. Medical Care, 45(6), 545–552.
- Johnston M., Carey R. N., Connell Bohlen L., Johnston D. W., Rothman A., de Bruin M., … Michie S. (2020). Linking behavior change techniques and mechanisms of action: Triangulation of findings from literature synthesis and expert consensus. Translational Behavioral Medicine, ibaa050, 1–17. doi:
- Jonsdottir H., Opjordsmoen S., Birkenaes A. B., Simonsen C., Engh J. A., Ringen P. A., … Andreassen O. A. (2013). Predictors of medication adherence in patients with schizophrenia and bipolar disorder. Acta Psychiatrica Scandinavica, 127(1), 23–33.
- Jose T. T., Bhaduri A., & Mathew B. (2003). A study of the factors associated with compliance or non-compliance to lithium therapy among the patients with bipolar affective disorder. Nursing Journal of India, 94(1), 9–11.
- Kamaradova D., Latalova K., Prasko J., Kubinek R., Vrbova K., Mainerova B., … Holubova M. (2016). Connection between self-stigma, adherence to treatment, and discontinuation of medication. Patient Preference and Adherence, 10, 1289–1298.
- Keck P. E., McElroy S. L., Strakowski S. M., Balistreri T. M., Kizer D. I., & West S. A. (1996). Factors associated with maintenance antipsychotic treatment of patients with bipolar disorder. The Journal of Clinical Psychiatry, 57(4), 147–151.
- Keck P. E., McElroy S. L., Strakowski S. M., Bourne M. L., & West S. A. (1997). Compliance with maintenance treatment in bipolar disorder. Psychopharmacology Bulletin, 33(1), 87–91.
- Kikkert M. J., Schene A. H., Koeter M. W., Robson D., Born A., Helm H., … Gray R. J. (2006). Medication adherence in schizophrenia: Exploring patients', carers' and professionals' views. Schizophrenia Bulletin, 32(4), 786–794. doi:
- Kraemer S., Minarzyk A., Eppendorfer S., Henneges C., Hundemer H.-P., Wilhelm S., & Grunze H. (2013). Comparably high retention and low relapse rates in different subpopulations of bipolar patients in a German non-interventional study. BMC Psychiatry, 13, 193.
- Kutzelnigg A., Kasper S., Kopeinig M., Chen C.-K., Fabian A., Pujol-Luna M. G., … Doby D. (2014). Compliance as a stable function in the treatment course of bipolar disorder in patients stabilized on olanzapine: Results from a 24-month observational study. Clinical and Translational Imaging, 2(1), 1–14.
- Lagard R., Keegan J., & Ward K. (2003). In-depth interviews. In J. Ritchie, & J. Lewis (Eds.), Qualitative research practice: A guide for social science students and researchers (pp. 138–139). London, UK: Sage.
- Landis J. R., & Koch G. G. (1977). The measurement of observer agreement for categorical data. Biometrics, 33(1), 159–174.
- Lingam R., & Scott J. (2002). Treatment non-adherence in affective disorders. Acta Psychiatrica Scandinavica, 105(3), 164–172. doi:
- Maczka G., Siwek M., Skalski M., Grabski B., & Dudek D. (2010). Patients' and doctors' attitudes towards bipolar disorder – Do we share our beliefs? Archives of Psychiatry and Psychotherapy, 12(2), 43–50.
- Manwani S. G., Szilagyi K. A., Griffin M. L., Weiss R. D., Hennen J., & Zablotsky B. (2007). Adherence to pharmacotherapy in bipolar disorder patients with and without co-occurring substance use disorders. Journal of Clinical Psychiatry, 68(8), 1172–1176.
- Michie S., Johnston M., Abraham C., Lawton R., Parker D., Walker A., & ‘Psychological Theory’ Group. (2005). Making psychological theory useful for implementing evidence based practice: A consensus approach. Quality & Safety in Health Care, 14(1), 26–33. doi: .
- Michie S., Johnston M., Francis J., & Hardeman W. (2008). From theory to intervention: Mapping theoretically derived behavioural determinants to behaviour change techniques. Applied Psychology, 57(4), 660–680.
- Millstein R. A., Celano C. M., Beale E. E., Beach S. R., Suarez L., Belcher A. M., … Huffman J. C. (2016). The effects of optimism and gratitude on adherence, functioning and mental health following an acute coronary syndrome. General Hospital Psychiatry, 43, 17–22. doi:
- Moher D., Liberati A., Tetzlaff J., Altman D. G., & The PRISMA Group. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Medicine, 6(7), e1000097. doi:.
- Morselli P. L., & Elgie R. (2003). GAMIAN-Europe*/BEAM survey I – Global analysis of a patient questionnaire circulated to 3450 members of 12 European advocacy groups operating in the field of mood disorders. Bipolar Disorders, 5(4), 265–278.
- Nagesh H. N., Kishore M. S., & Raveesh B. N. (2016). Assessment of adherence to psychotropic medications in a psychiatric unit of district hospital. National Journal of Physiology, Pharmacy and Pharmacology, 6(6), 581–585.
- National Institute of Health. (2014). Quality assessment tool for observational cohort and cross sectional studies. Retrieved May 5, 2020, from https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools.
- National Institute of Health and Care Excellence (NICE). (2009). Medicines adherence: Involving patients in decisions about prescribed medicines and supporting adherence. London: NICE.
- National Institute of Health and Care Excellence (NICE). (2014). Bipolar disorder: Assessment and management (clinical guideline, CG 185). London: nice.
- Nieuwlaat R., Wilczynski N., Navarro T., Hobson N., Jeffery R., Keepanasseril A., … Haynes R. B. (2014). Interventions for enhancing medication adherence. The Cochrane Database of Systematic Reviews, 2014(11), CD000011. doi: .
- Novick D., Montgomery W., Treuer T., Koyanagi A., Aguado J., Haro J. M., (2017). Comparison of clinical outcomes with orodispersible versus standard oral olanzapine tablets in nonadherent patients with schizophrenia or bipolar disorder. Patient Preference and Adherence, 11, 1019–1025.
- Perron B. E., Zeber J. E., Kilbourne A. M., & Bauer M. S. (2009). A brief measure of perceived clinician support by patients with bipolar spectrum disorders. Journal of Nervous & Mental Disease, 197(8), 574–579.
- Pope M., & Scott J. (2003). Do clinicians understand why individuals stop taking lithium? Journal of Affective Disorders, 74(3), 287–291.
- Prajapati A. R., Dima A., Clark A. B., Gant C., Gibbons C., Gorrod R., … Bhattacharya D. (2019). Mapping of modifiable barriers and facilitators of medication adherence in bipolar disorder to the theoretical domains framework: A systematic review protocol. BMJ Open, 9(2), e026980. doi:
- Priebe S., Bremner S. A., Lauber C., Henderson C., & Burns T. (2016). Financial incentives to improve adherence to antipsychotic maintenance medication in non-adherent patients: A cluster randomised controlled trial. Health Technology Assessment, 20(70), 121.
- QSR International Pty Ltd. (2018). Nvivo 12 for windows. NVivo qualitative data analysis software (computer software).
- Ralat S. I., Depp C. A., & Bernal G. (2018). Reasons for nonadherence to psychiatric medication and cardiovascular risk factors treatment among Latino bipolar disorder patients living in Puerto Rico: A qualitative study. Community Mental Health Journal, 54(6), 707–716. doi:
- Roe D., Goldblatt H., Baloush-Klienman V., Swarbrick M., & Davidson L. (2009). Why and how people decide to stop taking prescribed psychiatric medication: Exploring the subjective process of choice. Psychiatric Rehabilitation Journal, 33(1), 38–46.
- Rosa A. R., Marco M., Fachel J. M. G., Kapczinski F., Stein A. T., & Barros H. M. T. (2007). Correlation between drug treatment adherence and lithium treatment attitudes and knowledge by bipolar patients. Progress in Neuro-Psychopharmacology & Biological Psychiatry, 31(1), 217–224.
- Rosenblat J. D., Simon G. E., Sachs G. S., Deetz I., Doederlein A., DePeralta D., … McIntyre R. S. (2018). Factors that impact treatment decisions: Results from an online survey of individuals with bipolar and unipolar depression. The Primary Care Companion for CNS Disorders, 20(6), 18m02340. doi: .
- Rowland T. A., & Marwaha S. (2018). Epidemiology and risk factors for bipolar disorder. Therapeutic Advances in Psychopharmacology, 8(9), 251–269. doi:
- Sajatovic M., Bauer M. S., Kilbourne A. M., Vertrees J. E., & Williford W. (2006). Self-reported medication treatment adherence among veterans with bipolar disorder. Psychiatric Services (Washington, D.C.), 57(1), 56–62.
- Sajatovic M., Ignacio R. V., West J. A., Cassidy K. A., Safavi R., Kilbourne A. M., & Blow F. C. (2009). Predictors of nonadherence among individuals with bipolar disorder receiving treatment in a community mental health clinic. Comprehensive Psychiatry, 50(2), 100–107.
- Sajatovic M., Levin J., Fuentes-Casiano E., Cassidy K. A., Tatsuoka C., & Jenkins J. H. (2011). Illness experience and reasons for nonadherence among individuals with bipolar disorder who are poorly adherent with medication. Comprehensive Psychiatry, 52(3), 280–287.
- Salzmann-Erikson M., & Sjodin M. (2018). A narrative meta-synthesis of how people with schizophrenia experience facilitators and barriers in using antipsychotic medication: Implications for healthcare professionals. International Journal of Nursing Studies, 85, 7–18. doi:
- Scott J., & Pope M. (2002). Self-reported adherence to treatment with mood stabilizers, plasma levels, and psychiatric hospitalization. The American Journal of Psychiatry, 159(11), 1927–1929.
- Sharma S., Kumar N., Chakraborti S., Sinha S., Kumari S., & Gajendragad J. M. (2012). Prevalence and factors associated with medication compliance in Indian patients suffering from mental disorders. Tropical Doctor, 42(1), 28–31.
- Stentzel U., van den B. N., Schwaneberg T., Radicke F., Hoffmann W., Schulze L. N., … Langosch J. M. (2018). Predictors of medication adherence among patients with severe psychiatric disorders: Findings from the baseline assessment of a randomized controlled trial (TECLA). BMC Psychiatry, 18(1), 155.
- Strakowski S. M., Keck P. E. Jr, McElroy S. L., West S. A., Sax K. W., Hawkins J. M., … Bourne M. L. (1998). Twelve-month outcome after a first hospitalization for affective psychosis. Archives of General Psychiatry, 55(1), 49–55. doi: .
- Teter C. J., Falone A. E., Weiss R. D., Bakaian A. M., Tu C., & Ongur D. (2011). Medication adherence and attitudes in patients with bipolar disorder and current versus past substance use disorder. Psychiatry Research, 190(2), 253–258.
- Thompson K., Kulkarni J., & Sergejew A. A. (2000). Reliability and validity of a new medication adherence rating scale (MARS) for the psychoses. Schizophrenia Research, 42(3), 241–247. doi:
- Torres-Robles A., Wiecek E., Tonin F. S., Benrimoj S. I., Fernandez-Llimos F., & Garcia-Cardenas V. (2018). Comparison of interventions to improve long-term medication adherence across different clinical conditions: A systematic review with network meta-analysis. Frontiers in Pharmacology, 9, 1454. doi:
- The UCL Centre for Behaviour Change. (2019). The behaviour change taxonomy v1. Retrieved May 5, 2020, from https://www.bct-taxonomy.com/interventions.
- Vargas-Huicochea I., Huicochea L., Berlanga C., & Fresan A. (2014). Taking or not taking medications: Psychiatric treatment perceptions in patients diagnosed with bipolar disorder. Journal of Clinical Pharmacy and Therapeutics, 39(6), 673–679.
- Vazquez G. H., Holtzman J. N., Lolich M., Ketter T. A., & Baldessarini R. J. (2015). Recurrence rates in bipolar disorder: Systematic comparison of long-term prospective, naturalistic studies versus randomized controlled trials. European Neuropsychopharmacology: The Journal of the European College of Neuropsychopharmacology, 25(10), 1501–1512. doi:
- Velligan D. I., Weiden P. J., Sajatovic M., Scott J., Carpenter D., Ross R., … Expert Consensus Panel on Adherence Problems in Serious and Persistent Mental Illness. (2009). The expert consensus guideline series: Adherence problems in patients with serious and persistent mental illness. The Journal of Clinical Psychiatry, 70(Suppl 4), 1–46.
- Vieta E., Azorin J. M., Bauer M., Frangou S., Perugi G., Martinez G., & Schreiner A. (2012). Psychiatrists' perceptions of potential reasons for non- and partial adherence to medication: Results of a survey in bipolar disorder from eight European countries. Journal of Affective Disorders, 143(1–3), 125–130.
- Weiss R. D., Greenfield S. F., Najavits L. M., Soto J. A., Wyner D., Tohen M., & Griffin M. L. (1998). Medication compliance among patients with bipolar disorder and substance use disorder. Journal of Clinical Psychiatry, 59(4), 172–174.
- Younas M., Bradley E., Holmes N., Sud D., & Maidment I. D. (2016). Mental health pharmacists views on shared decision-making for antipsychotics in serious mental illness. International Journal of Clinical Pharmacy, 38(5), 1191–1199.
- Zeber J. E., Copeland L. A., Good C. B., Fine M. J., Bauer M. S., & Kilbourne A. M. (2008). Therapeutic alliance perceptions and medication adherence in patients with bipolar disorder. Journal of Affective Disorders, 107(1–3), 53–62.