Cobb Syndrome in an Indian Girl
- Sardana, Kabir MD
- Sehgal, Virendra N. MD
- Mahajan, Supriya MD
- Bhushan, Premanshu MD
A 4-year-old girl was noted to have a birthmark over the thoracolumbar region at birth. Her mother had experienced a normal pregnancy, labor, and delivery. The lesion gradually expanded in size, with associated swelling of the underlying skin. The patient visited a peripheral health center where an initial diagnosis of a skin-covered lumbar mass suggestive of a subcutaneous lipoma was considered. At 8 months, the child developed progressive weakness of the lower limbs and urinary and fecal incontinence. Examination of the affected area revealed a conspicuous 10 × 12-cm port-wine stain and swelling covering the back, between T5 and T12 (Figure 1). There was no apparent bruit, thrill, or raised temperature. There was a soft underlying mass suggestive of a lipoma. The child had severe spastic paraparesis in the lower extremities, with a very limited ability to lift her limbs, no muscle contractions or atrophy, with marked bladder/fecal dysfunction. She was examined by magnetic resonance imaging. Plain x-rays revealed a widening of the spinal canal with features suggestive of spina bifida. A Doppler study revealed a high-flow arteriovenous malformation. A T1-weighted magnetic resonance imaging scan of the thoracic and lumbar spine revealed high and low signal intensity associated with the T9–L2 vertebral bodies and T9–L2 paravertebral regions; enlargement of the spinal canal was noted, and the spinal cord was noted to be compressed (Figure 2A and B). The findings suggested vertebral, paravertebral, and spinal angiomas, with lipomyelo-meningocele and compression of the cord. Ultrasonography of the abdomen was normal. The parents were reluctant to undergo arteriography. Consequently, the patient was administered prednisolone p.o. at an initial dosage of 15 mg/d (2 mg/kg every 24 hours in divided doses, 4–6 hourly). Paraparesis partially improved with some regression of the port-wine stain. In view of the size of the underlying angioma and pressure effect, a consultation by pediatric neurosurgeons was performed. Endovascular embolization with surgical reduction of the lipomyelomeningocele was contemplated, but the associated risk and chance of recurrence/incomplete response proved to be a deterrent to the parents.
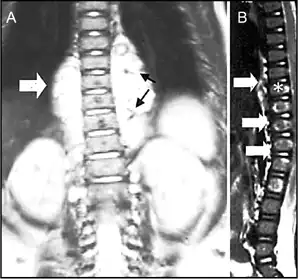
Figure 2
A) T1-weighted and B) gadolinium-enhanced magnetic resonance imaging scans revealing high and low signal intensity associated with the T9(*)–L2 vertebral bodies (suggesting vertebral angioma), T9–L2 paravertebral lesions (open arrows), and the T5–L3 spinal canal (arrowheads), suggesting a huge vascular malformation. Signal voids were obtained in the paravertebral angiomas, suggesting vascular malformation (arrows)

Figure 1
Port-wine stain with associated swelling, located between T5 and T12 on the back