WHAT IS ALREADY KNOWN ON THIS TOPIC
WHAT THIS STUDY ADDS
Sophisticated analyses of contemporary large administrative and health datasets collected routinely, using measures of absolute and relative inequalities.
First time a study of this size has reported on inequalities in prevalence of coexisting obesity and caries using Scottish data.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Early intervention, using established multiagency programmes which can collaborate to tackle non-communicable diseases as recommended by the WHO, is crucial to prevent coexisting conditions.
Ensuring national programmes reach children likely to develop coexisting obesity and caries experience and their families is essential for providing necessary support.
Background
Globally, inequalities in child oral health and childhood obesity pose a major public health challenge. Dental caries in primary dentition affects over 514 million children and 38.2 million children under the age of 5 years are affected by overweight or obesity, burdening healthcare systems and society. These conditions harm early-life health, quality of life and future education, particularly affecting vulnerable groups due to socioeconomic inequalities. As a consequence, an understanding of the drivers/determinants underpinning these inequalities is a strategic goal of the WHO. Some studies identify an association between childhood caries and obesity, likely due to the shared risk factors such as high sugar consumption. Systematic reviews provide conflicting information on the association between caries and obesity with the true relationship unknown due to methodological limitations of study designs, generally small sample sizes. Dental caries and obesity manifest early in childhood, share common risk factors, are sufficiently prevalent and in combination, could signal higher risk of multimorbidity in adulthood impacting quality of life and life expectancy, and challenging healthcare systems. Early identification and intervention in high-risk children could help prevent chronic conditions in later life. This study aims to quantify coexisting caries and obesity in children in Scotland between 2011/2012 and 2017/2018 and examine associated socioeconomic inequalities to identify the prevalence of children requiring further intervention and socioeconomic groups that require further support.
Methods
Study design and participants
Data from seven population-wide birth cohorts of children in primary 1 between 2011/2012 and 2017/2018 in Scotland were collated from two routine health databases held by Public Health Scotland (PHS).
Databases
National Dental Inspection Programme (NDIP) database annually surveys oral health in primary 1 (approximately 5 years old) children in local authority schools on an opt-out basis. Trained and standardised dental teams assess each child’s mouth and teeth.
Child Health Surveillance Programme–School (CHSP-S) collects data from Scotland’s annual body mass index (BMI) survey for primary 1 children in local authority schools on an opt-out basis, with optional participation for some private schools. Health professionals, typically school nursing teams, follow Royal College of Paediatrics and Child Health guidelines for reviews conducted throughout the academic year.
Definitions
Obvious caries experience (yes/no) was defined as the child having one or more of: abscess or infection, gross caries, obviously carious (into dentine) permanent or primary tooth, missing primary molar, evidence of restorations.
BMI SD scores (SDS) ( ) were computed using Cole’s UK 1990 references. Using epidemiological age-specific and sex-specific cut-offs, children in ≥95th centile (SDS circa ≥1.645) had obesity, centiles ≥85th and <95th (SDS circa ≥1.036 and 1.645) had overweight, centiles >2nd and <85th (SDS circa >−2 and <1.036) had healthy weight, and <2nd centile (SDS circa ≤−2) had underweight.
Children with both obesity and obvious caries experience were categorised as having coexisting obesity and caries experience and were compared with those with neither condition. Those with either condition were considered, though not reported here (see online supplemental figures 1–4).
SP110.1136/archdischild-2023-326587.supp1SP210.1136/archdischild-2023-326587.supp2SP310.1136/archdischild-2023-326587.supp3SP410.1136/archdischild-2023-326587.supp4
Area-based socioeconomic deprivation, based on the Scottish Index of Multiple Deprivation (SIMD) at a national level, used child home postcodes. SIMD assesses deprivation through 38 indicators across seven domains. The list of small areas (data zones) was ordered by deprivation and split into fifths. SIMD 1 represents the most deprived 20% and SIMD 5 represents the least deprived 20%. SIMD 2012 was used for academic years 2011/2012–2013/2014 and SIMD 2016 for 2014/2015–2017/2018 following PHS and CHSP-S guidelines.
Inclusion criteria
The cohort included primary 1 children aged 4.0–7.0 years old, with valid dental and BMI assessments from 2011/2012 to 2017/2018. NDIP had 401 054 children, but after exclusions (false ID matches, no examinations, age, missing deprivation, invalid outcomes, repeat examinations, duplicates), it comprised of 357 798 children (online supplemental figure 5). CHSP-S initially had 374 067 children. After exclusion (age, extreme BMI/height/weight SDS, missing deprivation), it comprised of 373 189 children (online supplemental figure 5). Linking the databases gave a cohort of 335 361 children who had a valid NDIP and CHSP-S assessment.
SP510.1136/archdischild-2023-326587.supp5
Statistical analysis
Analyses occurred in the National Health Service National Safe Haven, adhering to best practice guidance. R V.3.6.1 was employed for data cleaning and statistical analysis. Trends were examined in coexisting obesity and caries experience (defined as coexisting conditions) in children over 7 academic years (2011/2012–2017/2018) using line graphs, considering sex and area-based deprivation (SIMD).
To address inequalities comprehensively, Slope Index of Inequality (SII) and Relative Index of Inequality (RII) were calculated with 95% CIs to quantify absolute and relative inequalities in the prevalence of coexisting conditions. SII and RII were calculated via additive and multiplicative Poisson regression, respectively. The coexisting conditions rate (n=11 494) was used as the dependent variable, with the midpoint of the cumulative population in each socioeconomic fifth (measured by SIMD) as the independent variable, employing robust SEs. SII measures absolute inequality in the rate between those from the most and least deprived areas in terms of a rate difference, while RII represents the ratio of coexisting conditions in those from the most deprived areas compared with those from the least deprived areas. To assess trends, linear regression was performed, regressing SII and RII estimates against academic years as a continuous variable.
To assess coexisting condition risk over time, we employed a multinomial logistic regression model with four mutually exclusive outcomes, where coexisting conditions (n=11 494), caries experience only (n=90 895) and obesity only (n=21 466) as outcomes, compared with neither condition (n=211 506). This method provided a ‘clean’ reference category of neither condition rather than a ‘not caries or obesity’ reference category in a binary logistic model which could dilute the main contrast of interest. This produced parameter estimates which compared coexisting versus neither condition, caries experience only versus neither condition and obesity only versus neither condition. We used categorical independent variables: area-based deprivation (SIMD), sex, age and academic year. The final model included only the main effects of these variables. Adjusted ORs (aORs) were calculated by exponentiating model estimates, and 95% CIs were presented.
Results
A total of 335 361 children with valid data on caries experience (yes/no) and BMI status (underweight, healthy weight, overweight, obesity) were available. The seven cohorts represented 83.2% (n=46 417 of 55 769), 84.6% (n=48 222 of 57 021), 83.0% (n=49 369 of 59 490), 82.5% (n=49 349 of 59 796), 81.8% (n=47 840 of 58 497), 75.1% (n=46 334 of 61 695) and 79.7% (n=47 830 of 60 001) of the National Records for Scotland (NRS) population estimate for the 7 academic years, respectively. The reduction in population captured was distributed equally across the socioeconomic scale and for each sex, thus should have no effect on the results. The cohorts had a balanced sex split of 50.9% (n=170 745 of 335 361) males and 49.1% (n=164 616 of 335 361) females (table 1). The SIMD distribution favoured SIMD 1 (most deprived; 23.1%) and had the fewest in SIMD 5 (least deprived; 18.7%), aligning with NRS birth records. Caries experience prevalence declined since 2011/2012, while obesity prevalence remained steady, both exhibiting socioeconomic gradients. Children with caries experience had a higher likelihood of obesity than children with no caries experience (11.2% vs 9.2%), and among children with obesity, 34.9% had caries experience vs 29.8% with a healthy BMI (table 1).
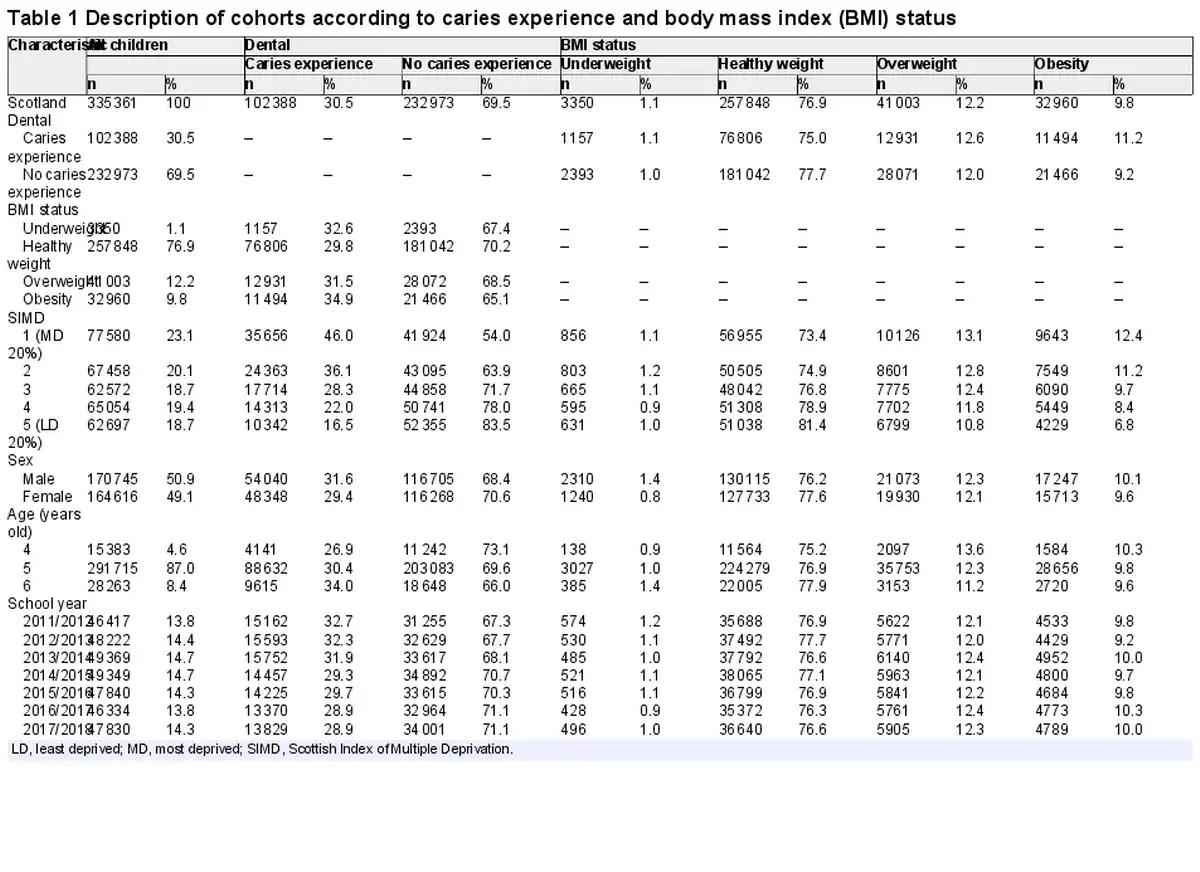
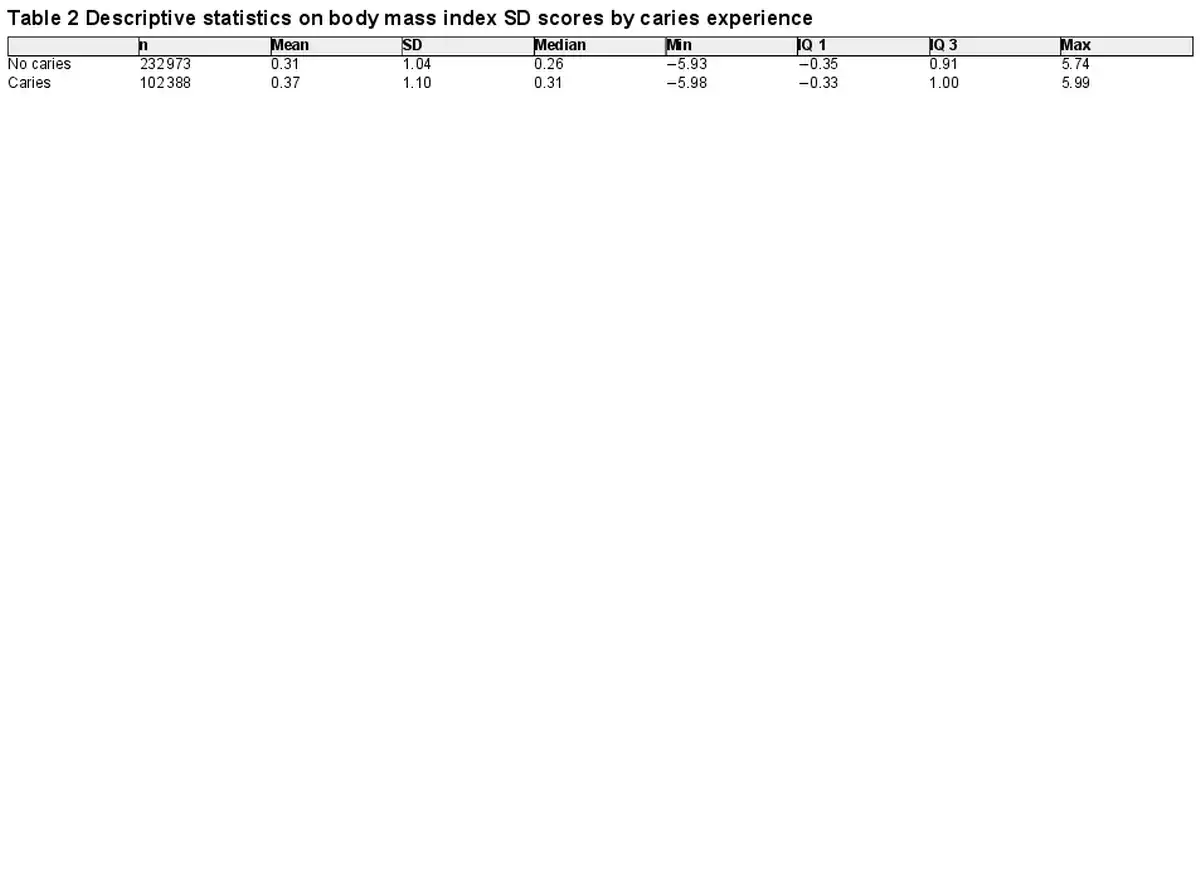
Overall, the mean BMI SDS was 0.33. In children with caries experience, it was slightly higher (0.37) than those without caries experience (0.31) (table 2). Children with caries had a wider range of BMI SDS values, with a lower minimum and higher maximum (table 2).
Prevalence of coexisting obesity and caries experience
Overall, coexisting conditions prevalence was 3.4% (n=11 494 of 335 361), which remained stable across the 7 academic years, with a 63.1% (n=211 506 of 335 361) prevalence of children with neither condition, which slightly increased over the 7 years. The trend is coexisting conditions held for both sexes with males and females maintaining 3.7% (2011/2012 n=870 of 23 717; 2017/2018 n=905 of 24 452) and 3.2% (2011/2012 n=736 of 22 700; 2017/2018 n=744 of 23 378) prevalence, respectively, in both 2011/2012 and 2017/2018 (online supplemental table 1). In 2011/2012, prevalence of coexisting conditions was 5.7% (n=605 of 10 614) in children from the most deprived areas (SIMD 1) vs 1.5% (n=126 of 8403) in children from the least deprived areas (SIMD 5), a 4.2% (n=479) difference. In 2017/2018, this gap widened to 4.6% (n=515), with a prevalence of 5.8% (n=624 of 10 749) in SIMD 1 and 1.2% (n=109 of 9381) in SIMD 5 (figure 1). Prevalence slightly increased with age, with 3.2% (n=493 of 15 383) at age 4, 3.4% (n=9960 of 291 715) at age 5 and 3.7% (n=1041 of 28 263) at age 6 years (online supplemental table 1).
SP610.1136/archdischild-2023-326587.supp6
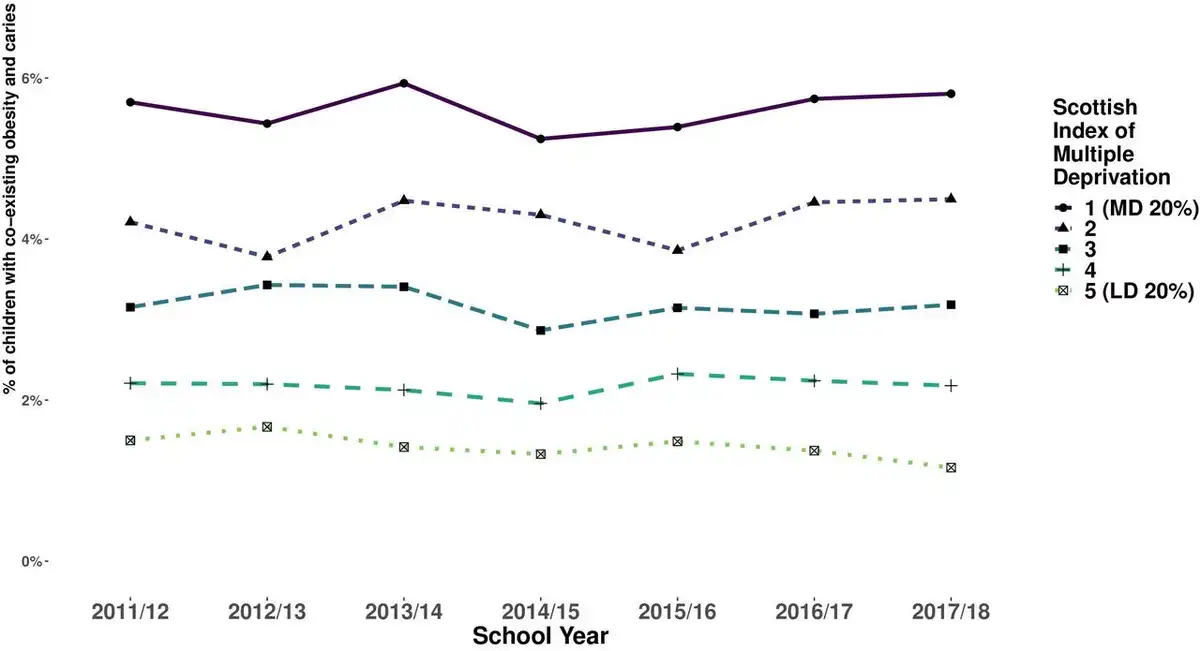
Figure 1
Prevalence of coexisting obesity and caries experience in 5-year-old schoolchildren in Scotland split by area-based deprivation (online supplemental table 1). LD 20%, least deprived 20%; MD 20%, most deprived 20%.
Inequalities in coexisting obesity and caries experience
For clarity, we present the results from the multinomial model for coexisting conditions versus neither condition in the main text of the results as the salient findings. For completeness, the other contrasts (caries only vs neither and obesity only vs neither) are provided in the online supplemental material.
SP710.1136/archdischild-2023-326587.supp7SP810.1136/archdischild-2023-326587.supp8
In a multivariable multinomial logistic regression model, adjusting for sex, age and academic year, children from the most deprived 20% of areas in Scotland have over six times the odds of coexisting obesity and caries compared with those in the least deprived 20% (aOR=6.63; 95% CI=6.16 to 7.14; p<0.001), showing a gradient across all SIMD fifths (figure 2). Males had slightly higher odds than females (aOR=1.16; 95% CI: 1.12 to 1.20; p<0.001), and odds increased with age (figure 2 and online supplemental table 2).
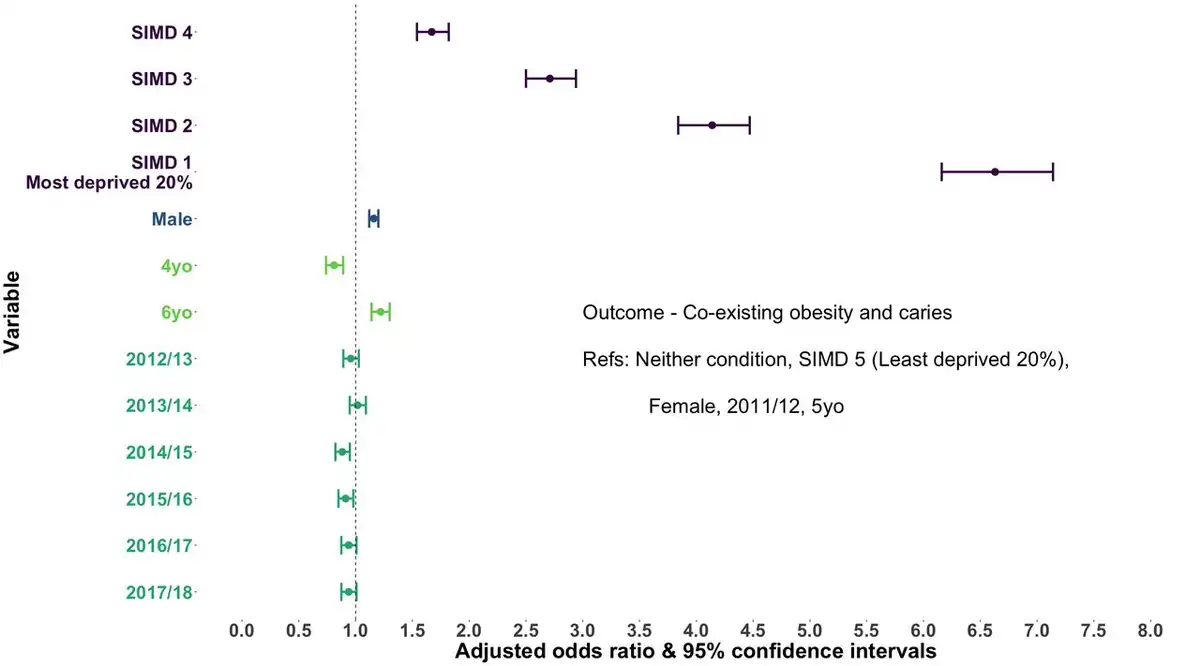
Figure 2
Adjusted ORs and 95% CIs for the risk of experiencing coexisting obesity and caries experience compared with experiencing neither condition for sex, age, academic year and socioeconomic deprivation (SIMD). SIMD, Scottish Index of Multiple Deprivation; yo, years old.
The absolute and relative indices of inequality for coexisting conditions remained stable, although large (figure 3 and online supplemental table 3). The SII was estimated at 5.0% (95% CI: 4.5% to 5.6%) in 2011/2012 and 5.8% (95% CI: 5.5% to 6.0%) in 2017/2018 (p slope=0.23). The RII was estimated to be 5.05 (95% CI: 4.48 to 5.69) in 2011/2012 and 6.25 (95% CI: 4.50 to 8.69) in 2017/2018, which although not a significant increase (p for slope=0.17), appears to be a rise over the study period.
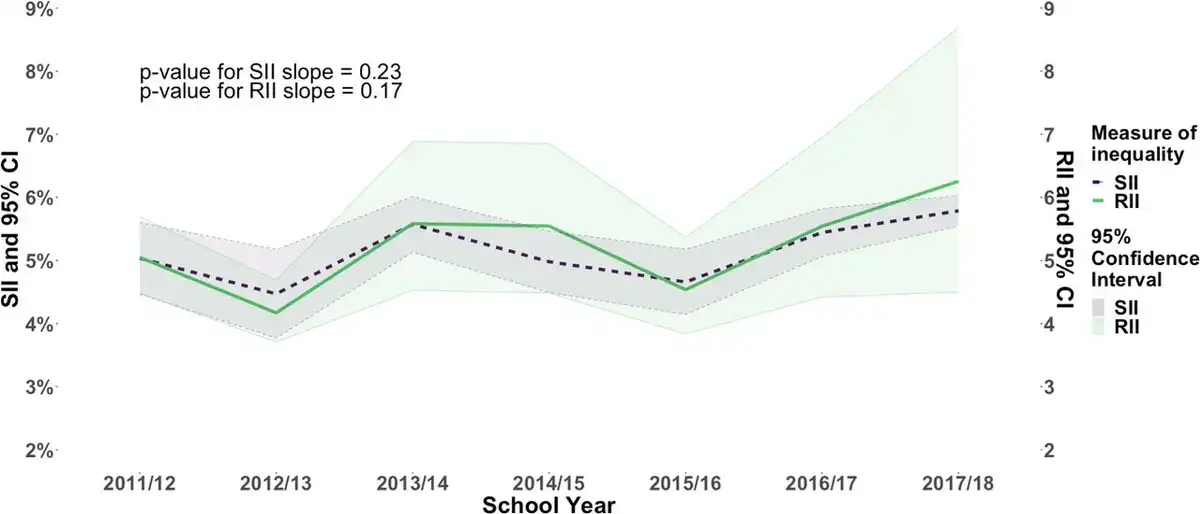
Figure 3
Slope Index of Inequality (SII) and Relative Index of Inequality (RII) for children with coexisting obesity and caries experience.
Discussion
This study revealed a persistent 3.4% prevalence of coexisting childhood obesity and caries experience in Scotland over nearly a decade, despite caries experience rates improving during the same period. These overall figures mask stark inequalities, with children living in the most deprived areas having over six times the odds of having coexisting conditions than those from the least deprived areas, an inequality that has endured over time.
To the best of our knowledge, no other study in Scotland or the UK has continuously examined coexisting conditions over this duration. Public Health England reported a 2.4% prevalence of coexisting conditions in children 5 years old in 2016/2017, lower than the 3.4% in Scotland. However, this discrepancy may stem from differences in consent protocols, with opt-in consent in England versus opt-out in Scotland, possibly favouring less deprived areas. A recent PhD thesis, based on the Born in Bradford Study, reported a 3.5% (n=6 of 171) prevalence among children 0–5 years old in 2014/2015, aligning with our findings, though this was a 1-year estimate with varying age groups and a limited sample from a specific area in England.
Few recent global studies have estimated the prevalence of coexisting conditions, with limited comparability. A US study from 2008, using 1999–2002 data, reported a 3.9% (~56 of 1449) prevalence in children 2–5 years old, focused solely on primary dentition. However, given the 9-year gap and US–Scotland differences, comparisons are difficult. A study from Greenland found a 3.8% (14 of 373) prevalence in children with a median age of 6.6 years old (2005–2007 births), with higher caries (57.1%) and lower obesity (5.1%) prevalence than this study. In 2013, in Greece, the prevalence was estimated at 0.5% in 2180 children aged 2.5–5.9 years old, with lower obesity (3.2%) and caries (10.0%), differing substantially from the prevalence identified in Scotland.
This study has found significantly large and consistent socioeconomic inequalities in the prevalence of coexisting conditions during the study period (2011–2018). These children with coexisting conditions have compounded needs and potential preventive interventions using the common risk factor approach could be developed. However, this group has not previously been identified as an important target/priority group in Scotland and there is a need to identify the risk predictors for having coexisting conditions in early childhood. To the authors’ best knowledge, there are no studies to estimate the inequalities in children with coexisting caries and obesity.
Our study exhibits both strengths and limitations. The data do not encompass all children attending private schools, which constitute around 5% of the student population, although these children are likely to be more affluent and less impacted. The data also only measure children who were in attendance on the day of inspection. Regarding health data, we relied on routine administrative health service data, which come with certain limitations in terms of detail. Obesity can be defined as an accumulation of excess body fat, rather than simply an increase in body weight. Given the challenge of directly measuring body fat in large population-based studies, a high BMI-for-age is commonly employed as an indirect indicator of elevated body fatness. However, relying on BMI-for-age as a substitute leads to a significant underestimation of actual obesity rates compared with a measurement of excessive fatness. This suggests that the true prevalence of obesity in Scotland is likely higher than the reported estimates, which were derived from BMI-for-age calculations. Thus, our presented figures for obesity prevalence among children 5 years old in Scotland are likely conservative. Personal socioeconomic data at the individual level were not available within the regular administrative data. Consequently, we relied on area-based deprivation indicators. This approach has its limitations, as it involves drawing conclusions about individuals based on group-level data (ie, the ecological fallacy) and does not account for variations in individual-level risk factors and disease prevalence within residential areas. However, area-level measures are very commonly used as an indicator of socioeconomic position. These limitations are offset by their broad coverage, high quality and comprehensiveness. In our analysis, we used dental caries outcome data from NDIP. These data, obtained through ‘basic’ inspections, yielded similar results to data from detailed epidemiological inspections, which encompass more comprehensive information on dental caries experiences (d3mft) and are conducted on a 20% subset of the population by trained and standardised examiners using the criteria established by the British Association of Community Dentistry. The prevalence of obvious caries experience in children 5 years old was approximately 30.6% (2016) and 28.9% (2018) based on basic inspections, while it was 30.1% (2016) and 29.6% (2018) from detailed epidemiological inspections. The process of linking education and health records through probabilistic matching is considered robust and has been previously validated with an accuracy rate of 99%. Our analysis was comprehensive and accounted for key confounding factors such as socioeconomic status and age when evaluating caries and obesity outcomes.
Conclusions
We observed a consistent prevalence of coexisting obesity and caries experience in children in primary 1 (approximately 5 years old) in Scotland from 2011 to 2018, with large stubborn socioeconomic inequalities. These children face heightened risk of future chronic diseases and multimorbidity, bearing economic and societal burdens. Early intervention, using established multiagency programmes which can collaborate to tackle non-communicable diseases as recommended by WHO, is crucial to prevent coexisting conditions. Ensuring national programmes reach children likely to develop coexisting obesity and caries experience and their families is essential for providing necessary support.
The authors would like to acknowledge the support of the eDRIS Team (Public Health Scotland) for their involvement in obtaining approvals, provisioning and linking data and the use of the secure analytical platform within the National Safe Haven.
X @stewart_ryan3
Contributors AS, LMDM and DC conceived the idea of this study. AS, DC, LMDM and RS designed the study. DC and AS prepared data requests and study approvals and data sharing agreements. RS undertook data management. RS with AS performed analysis and prepared figures and tables. AS and DC prepared first draft of the manuscript. RS prepared further drafts of the manuscript. AS is guarantor.
Funding Glasgow Children’s Charity (St Andrew’s Society of New York) PhD studentship and Scottish Government Childsmile monitoring and evaluation support.
Disclaimer The study funder had no role in study design, data collection, data analysis, data interpretation or writing of the report.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
References
- 1. World Health Organization. Global oral health status report: towards universal health coverage for oral health by 2030, 2022. Available: https://www.who.int/publications/i/item/9789240061484
- 2. World Health Organization. Obesity and overweight. 2021. Available: https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight
- 3. World Health Organization. Sugar and dental Caries. 2017. Available: https://apps.who.int/iris/bitstream/handle/10665/259413/WHO-NMH-NHD-17.12-eng.pdf;jsessionid=232F2E1BB44A393BE5CA1C9F7291B73A?sequence=1
- 4. Scottish Parliament Information Centre. Obesity in Scotland. 2015. Available: http://www.parliament.scot/ResearchBriefingsAndFactsheets/S4/SB_15-01_Obesity_in_Scotland.pdf
- 5. Weihrauch-Blüher S, Wiegand S. Risk factors and implications of childhood obesity. Curr Obes Rep 2018;7:254–9. doi:10.1007/s13679-018-0320-0
- 6. Botelho J, Mascarenhas P, Viana J, et al. An umbrella review of the evidence linking oral health and systemic Noncommunicable diseases. Nat Commun 2022;13:7614. doi:10.1038/s41467-022-35337-8
- 7. Hayden C, Bowler JO, Chambers S, et al. Obesity and dental Caries in children: a systematic review and meta-analysis. Community Dent Oral Epidemiol 2013;41:289–308. doi:10.1111/cdoe.12014
- 8. Hooley M, Skouteris H, Boganin C, et al. Body mass index and dental Caries in children and adolescents: a systematic review of literature published 2004 to 2011. Syst Rev 2012;1:57. doi:10.1186/2046-4053-1-57
- 9. Alshihri AA, Rogers HJ, Alqahtani MA, et al. Association between dental Caries and obesity in children and young people: A narrative review. Int J Dent 2019;2019:9105759. doi:10.1155/2019/9105759
- 10. NHS National Services Scotland. National Dental Inspection Programme. Edinburgh, 2018. Available: https://www.scottishdental.org/wp-content/uploads/2018/10/2018-10-23-NDIP-Report.pdf
- 11. Information Services Division Scotland. Body Mass Index of Primary 1 Children in Scotland School Year 2017/18, 2018. Available: https://www.isdscotland.org/Health-Topics/Child-Health/Publications/2018-12-11/2018-12-11-P1-BMI-Statistics-Publication-Report.pdf
- 12. Royal College of Paediatrics and Child Health. UK-WHO growth charts - guidance for health professionals 2020, 2020. Available: https://www.rcpch.ac.uk/resources/uk-who-growth-charts-guidance-health-professionals
- 13. Cole TJ, Freeman JV, Preece MA. Body mass index reference curves for the UK, 1990. Arch Dis Child 1995;73:25–9. doi:10.1136/adc.73.1.25
- 14. The Scottish Government. The Scottish Index of Multiple Deprivation 2016, 2016. Available: https://www.gov.scot/publications/scottish-index-multiple-deprivation-2016
- 15. The Scottish Government. The Scottish Inde of Multiple Deprivation 2012, 2012. Available: https://www.gov.scot/publications/scottish-index-multiple-deprivation-2012-executive-summary
- 16. Information Services Division Scotland. n.d. Deprivation guidance for analysts. National services Scotland. Available: https://www.isdscotland.org/Products-and-Services/GPD-Support/Deprivation/SIMD/_docs/PHI-Deprivation-Guidance.pdf
- 17. Public Health Scotland. eDRIS Products and Services - NHS National Safe Haven, 2023. Available: https://www.isdscotland.org/Products-and-Services/eDRIS
- 18. Benchimol EI, Smeeth L, Guttmann A, et al. The reporting of studies conducted using observational routinely-collected health data (RECORD) statement. PLOS Med 2015;12:e1001885. doi:10.1371/journal.pmed.1001885
- 19. Gilbert R, Lafferty R, Hagger-Johnson G, et al. GUILD: guidance for information about linking data SETS. J Public Health (Bangkok) 2018;40:191–8. doi:10.1093/pubmed/fdx037
- 20. R Core Team. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing, 2023. Available: https://www.R-project.org
- 21. Moreno-Betancur M, Latouche A, Menvielle G, et al. Relative index of inequality and slope index of inequality: a structured regression framework for estimation. Epidemiology 2015;26:518–27. doi:10.1097/EDE.0000000000000311
- 22. Mackenbach JP, Kunst AE. Measuring the magnitude of socio-economic inequalities in health: an overview of available measures illustrated with two examples from Europe. Soc Sci Med 1997;44:757–71. doi:10.1016/s0277-9536(96)00073-1
- 23. National records Scotland. Birth Time Series Data 2019. Available: https://www.nrscotland.gov.uk/statistics-and-data/statistics/statistics-by-theme/vital-events/births/births-time-series-data
- 24. Macpherson L, Conway D, McMahon A, et al. Report of the 2018 detailed inspection programme of primary 1 children and the basic inspection of primary 1 and primary 7 children. 2018. Available: https://www.isdscotland.org/Health-Topics/Dental-Care/Publications/2018-10-23/2018-10-23-NDIP-Report.pdf
- 25. Public Health England. The relationship between dental caries and body mass index: Child level analysis, 2019. Available: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/844121/BMI_dental_caries.pdf
- 26. Conway DI, McMahon AD, Smith K, et al. Socioeconomic factors influence selection and participation in a population-based case-control study of head and neck cancer in Scotland. J Clin Epidemiol 2008;61:1187–93. doi:10.1016/j.jclinepi.2007.12.012
- 27. Roberts BW, Yao J, Trzeciak CJ, et al. Income disparities and Nonresponse bias in surveys of patient experience. J Gen Intern Med 2020;35:2217–8. doi:10.1007/s11606-020-05677-6
- 28. Born in Bradford. 2017. Available: https://borninbradford.nhs.uk
- 29. Uerlich M. Obesity and Dental Caries in Children: Are There More Common Determinants than Diet? University of Sheffield, 2020.
- 30. Kopycka-Kedzierawski DT, Auinger P, Billings RJ, et al. Caries status and overweight in 2- to 18-year-old US children: findings from national surveys. Community Dent Oral Epidemiol 2008;36:157–67. doi:10.1111/j.1600-0528.2007.00384.x
- 31. Madsen SS, Wetterstrand VJR, Pedersen ML. Dental Caries and weight among children in Nuuk, Greenland, at school entry. Int J Circumpolar Health 2017;76:1311535. doi:10.1080/22423982.2017.1311535
- 32. Pikramenou V, Dimitraki D, Zoumpoulakis M, et al. Association between dental Caries and body mass in preschool children. Eur Arch Paediatr Dent 2016;17:171–5. doi:10.1007/s40368-016-0222-3
- 33. Sheiham A, Watt RG. The common risk factor approach: a rational basis for promoting oral health. Community Dent Oral Epidemiol 2000;28:399–406. doi:10.1034/j.1600-0528.2000.028006399.x
- 34. Watt RG. Social determinants of oral health inequalities: implications for action. Community Dent Oral Epidemiol 2012;40 Suppl 2:44–8. doi:10.1111/j.1600-0528.2012.00719.x
- 35. Javed A, Jumean M, Murad MH, et al. Diagnostic performance of body mass index to identify obesity as defined by body Adiposity in children and adolescents: a systematic review and meta-analysis. Pediatr Obes 2015;10:234–44. doi:10.1111/ijpo.242
- 36. Reilly JJ, Kelly J, Wilson DC. Accuracy of simple clinical and Epidemiological definitions of childhood obesity: systematic review and evidence appraisal. Obes Rev 2010;11:645–55. doi:10.1111/j.1467-789X.2009.00709.x
- 37. Diouf A, Adom T, Aouidet A, et al. Body mass index vs deuterium dilution method for establishing childhood obesity prevalence, Ghana, Kenya, Mauritius, Morocco, Namibia, Senegal, Tunisia and United Republic of Tanzania. Bull World Health Organ 2018;96:772–81. doi:10.2471/BLT.17.205948
- 38. Clelland D, Hill C. Deprivation, policy and Rurality: the limitations and applications of area-based deprivation indices in Scotland. Local Economy 2019;34:33–50. doi:10.1177/0269094219827893
- 39. Pine CM, Pitts NB, Nugent ZJ. British Association for the study of community dentistry (BASCD) guidance on the statistical aspects of training and calibration of Examiners for surveys of child dental health. A BASCD coordinated dental epidemiology programme quality standard. Community Dent Health 1997;14:18–29.
- 40. Wood R, Clark D, King A, et al. Novel cross-Sectoral linkage of routine health and education data at an all-Scotland level: a feasibility study. Lancet 2013;382:S10. doi:10.1016/S0140-6736(13)62435-6