Introduction
The function of acoustic transfer in the ear canal is determined by the sound transmission properties of the middle ear. The middle ear characteristics vary among populations, and factors such as age, gender, and ethnicity affect it [Shahnaz et al., 2013]. In any audiological assessment, improving the sensitivity and specificity of the test is the main goal. Shahnaz et al. [2013] suggest three methods to accomplish those standards: (a) adjusting the criterion level, (b) utilizing instrument-specific norms, and (c) using population-specific norms. A test’s specificity and sensitivity can be improved by adjusting the criterion value, which is the criterion that is used to determine whether an ear is normal or abnormal. Another way in which a test’s sensitivity and specificity may be altered is by using instrument-specific norms. Shahnaz and Bork [2008] analyzed whether the Virtual 310 System and the GSI Tympstar Middle Ear Analyzer System (Grason-Stadler, Eden Prairie, MN, USA) would generate comparable tympanograms and whether the two instruments were comparable in the detection of otosclerosis. It was found that some differences existed between the two systems on measurements of tympanometry features like admittance (Ad) and resonance frequency (RF). If the use of instrument specific norms does not result in improved sensitivity and specificity, then instrument-specific norms are not warranted because the test’s predictive value is not improved [Shahnaz and Bork, 2008]. The final procedure to improve a test’s sensitivity and specificity is by applying population-specific norms. One of the major works on this topic was done by Shahnaz and Davis by gathering ethnicity-specific norms (Caucasian vs. Chinese) for conventional 226-Hz tympanometric measures features. It was found that the use of ethnicity-specific norms resulted in improvements in test sensitivity and specificity [Shahnaz and Davies, 2006].
To distinguish sensorineural from conductive conditions, the middle ear function should be assessed. Wideband tympanometry (WBT) is a noninvasive, rapid, and accurate way of utilizing the wideband click as the probe tone among frequencies from 0.2 kHz up to 8 kHz to assess the middle ear function. The WBT provides measurements of both absorbance and reflectance, making this assessment of middle ear function more precise than multifrequency or conventional tympanometry [Hunter and Margolis, 1997; Sanford et al., 2013]. Assessments in newborns using a 226-Hz probe tone are insensitive to conductive conditions [Hunter and Margolis, 1992; Baldwin, 2006; Alaerts et al., 2007]. Tympanograms recorded from newborn infants are often very different from those obtained from older infants, children, and adults mainly because of ear canal flaccidity in newborns. In neonate ears with confirmed middle ear disease, 226-Hz tympanograms may not provide accurate diagnostic information. In addition, the variability of 226-Hz tympanometry in young infants because of the presence of M-shaped or notched patterns casts doubt on the clinical utility of these measures for newborns [Hunter and Margolis, 1992]. In most nations, universal newborn hearing screening programs (UNHS) have been undertaken. False-positive results during UNHS are frequently caused by middle ear problems such as otitis media with effusion. In their first year of life, more than half of all children are estimated to have otitis media with effusion [Physicians and Effusion, 2004]. In infants and young children, the feasibility of 678 and 1,000 Hz tympanometry (high-frequency tympanometry, HFT) was investigated and normative data were presented [Kei et al., 2003]. They concluded that tympanometry at 1,000 Hz provides more information on transient conductive hearing loss and lowers false-positive results in UNHS. Evidence has accumulated that tympanometry using a higher probe tone frequency (e.g., 1,000 Hz) is more sensitive to middle ear status, compared with 226-Hz tympanometry, in infants less than 4–6 months old (in these ages the use of high frequency 1,000 Hz (1 kHz) tympanometry has been recommended) [Hoffmann et al., 2013].
WBT has been presented as a reliable approach for assessing the health of the middle ear and its transmission system. WBT has been shown in studies to be a more sensitive diagnostic test for middle ear diseases and conductive hearing loss than traditional 226-Hz tympanometry. WBT has the benefit of being less sensitive to probe placement in the ear canal than traditional tympanometry, especially at higher frequencies [Shahnaz and Bork, 2006]. Additionally, WBT provides Ad-based evaluation up to a frequency of 10 kHz in adults and 20 kHz in infants. In the absence of normative and disease-specific data, this technique has not become widely used [Özgür et al., 2016]. Nevertheless, WBT or wideband acoustic immittance is an effective and desirable measure of conductive conditions in newborns and adults [Sanford and Brockett, 2014; Aithal et al., 2015].
Recently, there has been an increment in the utilization of WBT, which highlights the importance of collecting population-based normative data as a necessary step in the standardization of this instrument, as well as for its clinical application [Feeney et al., 2003]. Normative data are collected to improve the test’s sensitivity and specificity. It will be possible to improve the sensitivity and specificity of the tests by implementing population-specific norms. Hence, the abnormality of an ear can be determined more accurately. This will lead to fewer false alarms and more disordered ears will be correctly identified as being disordered [Shahnaz et al., 2013; Polat et al., 2015].
Recently, several studies have been done on the usage of WBT in various pathologies. However, there are not enough studies of normative data for WBT. In Shahnaz et al. [2013]’s study, the normative data between Caucasian and Chinese young adults differed significantly, with Caucasian subjects showing much greater reflectance at high frequencies. This result supports the idea that more ethnicity-based studies need to be addressed [Shahnaz et al., 2013].
In light of the lack of studies about normative WBT values, further measurements are needed. The aim of this study was therefore to collect normative data for WBT and absorbance values in young Iranian adults regarding the impact of ethnicity, gender, and aging.
Materials and Methods
Subjects
A total of 202 ears were analyzed from 101 participants. There were 43 male participants (42.6%) and 58 female participants (57.4%) between the ages of 19 and 29. All the subjects were from the Iranian race. This research was approved by the Local Ethical Committee and participants provided their informed consent. All volunteers signed an informed consent form before undergoing otoscopic examination, pure-tone audiometry, and WBT.
Inclusion and Exclusion Criteria
To be included in this study, participants had to have (a) present pure-tone audiometric thresholds better than 15 dB HL at octave frequencies between 250 and 8,000 Hz, (b) air-bone gaps were no greater than 15 dB HL between 250 and 4,000 Hz, (c) no history of hearing loss, otologic surgery, and no common cold should be provided, and (d) no significant tympanic membrane or external ear abnormalities like excessive cerumen revealed by otoscopic examination. Any individual with tinnitus, middle ear, or external ear canal pathologies diagnosed by the ear, nose, and throat (ENT) physician was excluded from this study. In addition, anyone with a history of long-term exposure to loud noises was excluded.
Instrumentation and Calibration
Pure-tone audiometry of all the subjects in this study was tested utilizing a clinical audiometer (AC40) Interacoustics Assens (Denmark) calibrated biologic manner according to American National Standards Institute criteria (re: S3.6-2010). TDH-39 earphones were used in a soundproof room for measurements that were calibrated according to criteria. Furthermore, the TDH-39 earphones were used in a soundproof room for measurements were calibrated using artificial ear (coupler) methods according to American National Standards Institute criteria (re: S3.6-2010). Before each subject’s recordings were made, the WBR equipment was calibrated using the four-cavity calibration device that has been invented for this purpose. Each participant was fitted with the proper ear-tip size. The Titan WBT device (Interacoustics; Assens, Denmark) was used to evaluate all candidates. A clinician conducted calibration before the first measurement of WBT in a silent room at tympanometric peak pressure (TPP) at octave frequencies between 226 and 8,000 Hz.
Procedure
If the subjects met the inclusion criteria, a standard 226-Hz tympanogram was recorded. Values of equivalent ear canal volume (Veq: a measure of the equivalent volume of air in front of the measuring probe, and it is only an accurate estimate of the volume in front of the probe when it is constrained by precise geometric restrictions.) [Noh and Lee, 2012], Ad (the highest amount of acoustic energy the middle ear system can absorb) [Onusko, 2004], TPP (the tympanometric peak, or point of greatest Ad, is the highest point in the tympanometric pattern on the y-axis. The ear canal and middle ear pressures are equivalent at this stage) [Shurin et al., 1977], gradient (G: a metric that describes the slope of a tympanometric form near its peak, which describes the relationship of its height to its width. Gs of less than 0.2 are regarded as unusually low and have been linked to the presence of middle ear fluid) [Camboim et al., 2012], RF (the frequency at which the interplay of mass and stiffness components controlling the middle ear is neutralized. Multifrequency tympanometry may be used to determine this frequency, and the normative value for adults is between 800 and 1,200 Hz) [André et al., 2012], energy absorbance (EA: the amount of energy conveyed through the middle ear system from a click sound) [Lilly and Margolis, 2013], maximum absorbance frequency, and absorbance percentage according to frequency were calculated. Also, OtoAccess ver. 1.2.1 (Interacoustics; Assens, Denmark) data-recording software was used to record the data and calculate the outcomes.
Recording Approach
There are different approaches to determining WBT, including measuring ambient pressure, TPP, and pressure sweep methods. There are different opinions about which methods are most reliable and valid. Some believe that WBT should be measured as TPP to provide a more accurate differential diagnosis of patients with middle ear diseases [Feeney et al., 2014]. In addition, there is a low inter-subject variance in TPP mode compared to ambient pressure. Shahnaz et al. [2013] have concluded that measuring WBT in TPP mode is more useful when the middle ear pressure is not 0. The measurement of WBT in TPP mode is considered to have a higher degree of test-retest reliability than ambient pressure. Especially with descending pressure sweeps, more accurate results are obtained than when using ambient methods [Feeney et al., 2017]. Therefore, this study was conducted at TPP since it appears that measuring WBT using TPP provides more reliable results than other methods.
Statistical Analysis
In this paper, the priority of the authors was investigating the influence of ethnicity, gender, and aging (dependent variable) on EA (independent variable). According to other published normative data studies in this field [Shahnaz and Davies, 2006; Polat et al., 2015], all the authors hypothesized that there should be a meaningful correlation between the impact of ethnicity, gender, and aging (dependent variable) on the EA (independent variable). Comparing the EA, RF, Veq, TPP, Ad, and G between two genders (men and women) and their correlations were the second goal of our study. Gender was assumed as the independent variable and all mentioned factors (EA, Veq, TPP, Ad, and G) were considered dependent variables for the second goal of this research.
For statistical analysis, SPSS 18 software was used (SPSS Inc.; Chicago, IL, USA). First, The Kolmogorov-Smirnov test was utilized to check out the null hypothesis that a normal distribution of variables exists in men and women.
Second, the Wilcoxon Signed-Rank test (a nonparametric statistical test that compares two paired groups. The test essentially calculates the differences between sets of pairs and analyzes these differences to establish if they are statistically significantly different from one another) was done for comparing dependent variables (RF, Veq, TPP, Ad, and G) of right and left ears in each gender. The Mann-Whitney U test (which is used to compare differences between two independent groups when the dependent variable is either ordinal or continuous but not normally distributed) was conducted for between-group (among men and women) comparisons of dependent variables regarding any correlations. Finally, the null hypothesis was considered the similarity and correlation of obtained values in right and left ears, inter and between each, group, and the p < 0.05 value was considered to be significant.
Results
To collect normative data, 101 subjects (19–29 years of age) of the Iranian race were evaluated (53 females and 48 males). The mean height, weight, and age of these subjects can be seen in the descriptive Table 1. In the Mann-Whitney U test, there was no significant relationship between the tested ear and absorbance values at any frequency (p > 0.05).
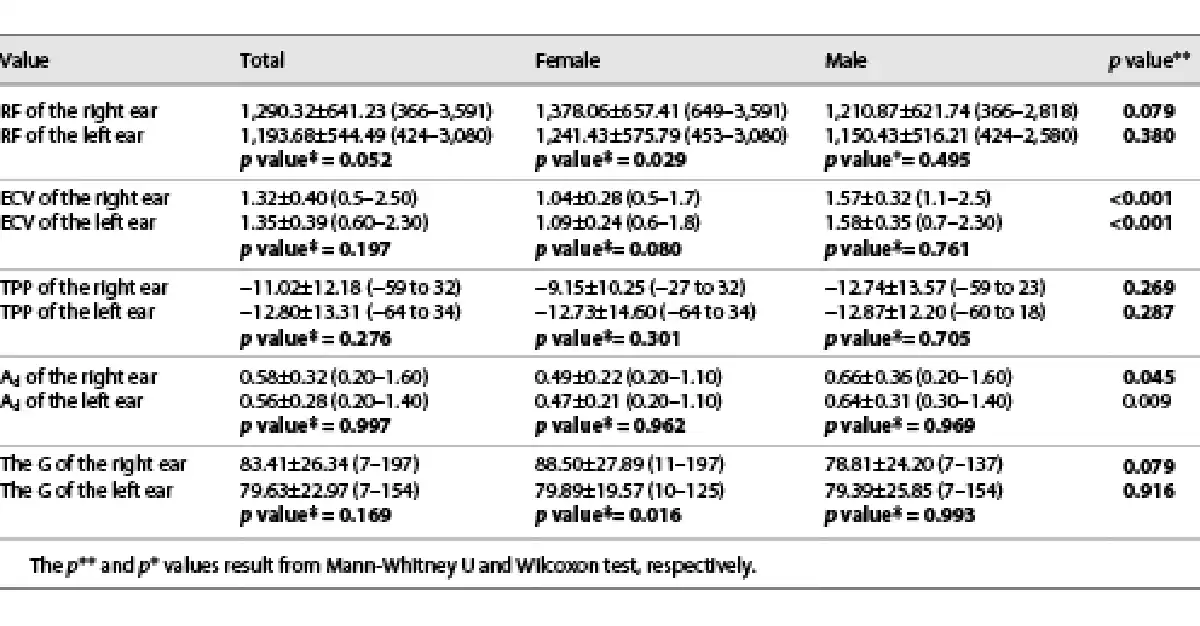
We measured the RF, Veq, TPP, Ad, and G values for all the subjects in this study at a standard single frequency of 226 Hz for investigating the differences and the correlations between mentioned values in both genders and inter each group. RF, Veq, TPP, Ad, and G and statistical analysis for male and female participants are summarized in Table 2. According to the statistical analysis of the Wilcoxon Signed-Rank test that can be shown in Table 2, the null hypothesis (similarity of dependent values between ears in each gender group) was established for the RF and the G of right and left ears of females (p < 0.05) and remnant values in each group were different between ears and no similarities were found (p > 0.05). It should be mentioned from the data in Table 2, the Mann-Whitney U test results showed that there was a significant correlation (similarity) in Ad and Veq between male and female subjects in both right and left ears (p < 0.05). The difference in anatomic size between males and females can also cause differences in their Veq values [Shahnaz and Bork, 2006; Shahnaz and Davies, 2006].
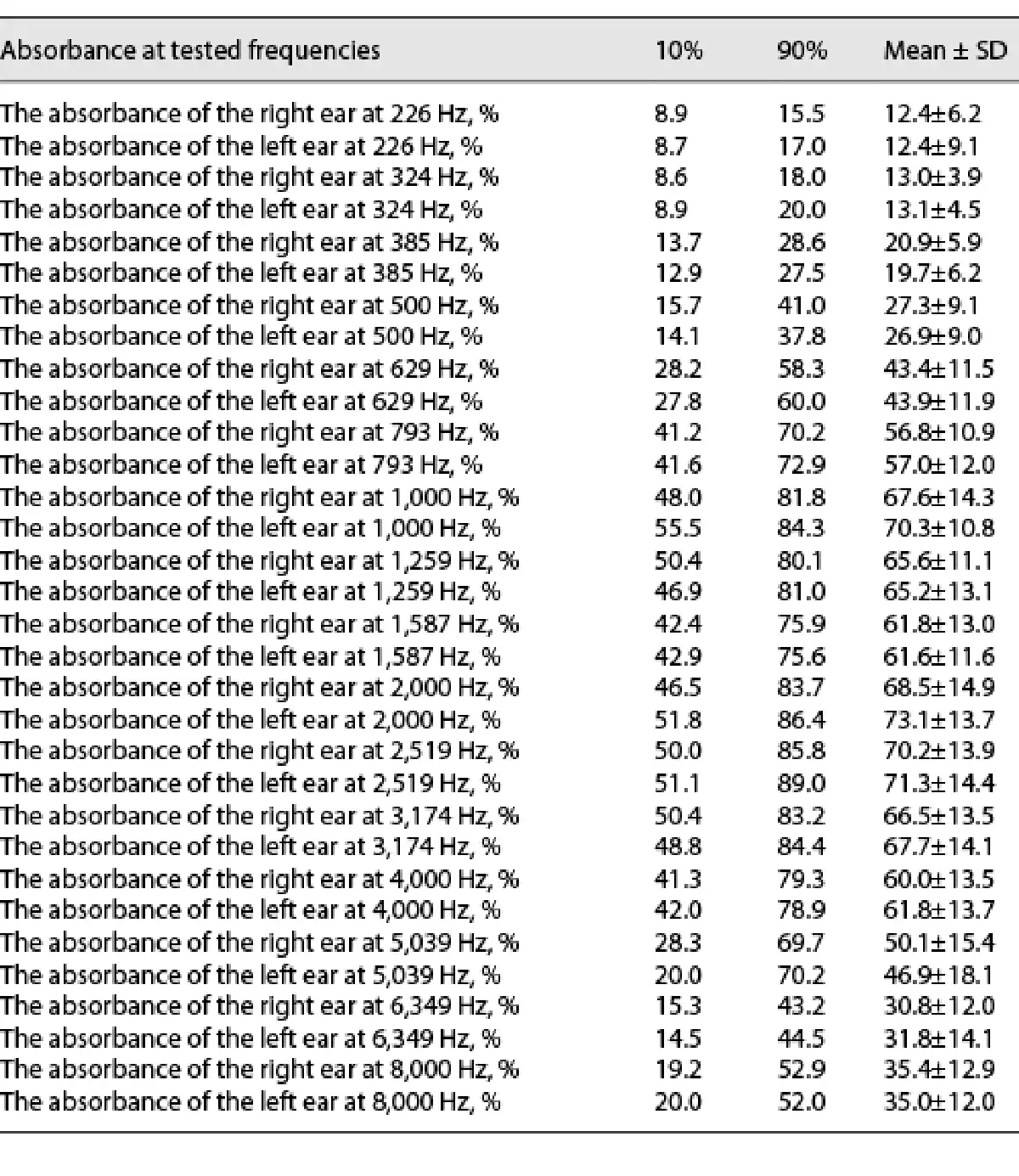
It has been manifested by the results of the Kolmogorov-Smirnov test that the distribution of EA in male and female participants was not normal. For this reason, the Mann-Whitney U test was used to investigate the correlation between EA and gender. It has been presented in Table 3, the EA amounts are shown at different frequencies with the 10th, 90th, and average percentiles, respectively. In both ears, the amount of EA increases with increasing frequency, both in the average and in the 10th and 90th percentiles. Also, it has a sharp increase in frequencies between 1,000 Hz and 2,000 Hz (the highest value). From frequency 2,519 Hz, the EA value decreases with increasing frequency, and a slight increase of 8,000 Hz is shown in comparison with previous frequencies. The EA values are highest at frequencies of 1,000 Hz, 2,000 Hz, and 2,519 Hz. The lowest value of EA is at 226 Hz.
Changes in EA in the 10th, 50th, and 90th percentiles, and the average can be manifested in Figure 1. The correlation between Table 3 and Figure 1 seems to be quite strong. EA peaks are visible at frequencies 1,000 Hz and 2,000 Hz (the highest value). In the range of 500–1,000 Hz, the G of the graph shows a steep increase. As the frequency of 3,174 Hz rises, the slope begins to descend and at 6,349 Hz there is a sudden drop in the EA value, but between 8,000 Hz and 9,000 Hz, there is a slight increase.
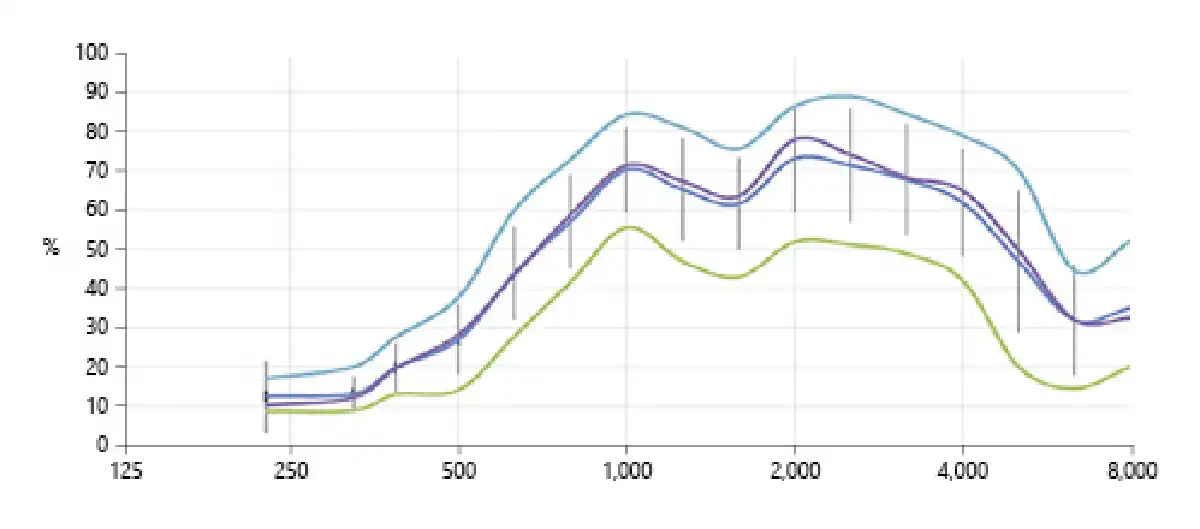
Fig. 1
The mean absorbance values across the 250–8,000 Hz frequencies bands for both men and women groups (from top to bottom; pale blue colored line: 90th percentile, purple colored line: 50th percentile, blue colored line: average at peak, and green colored line shows 10th percentile).
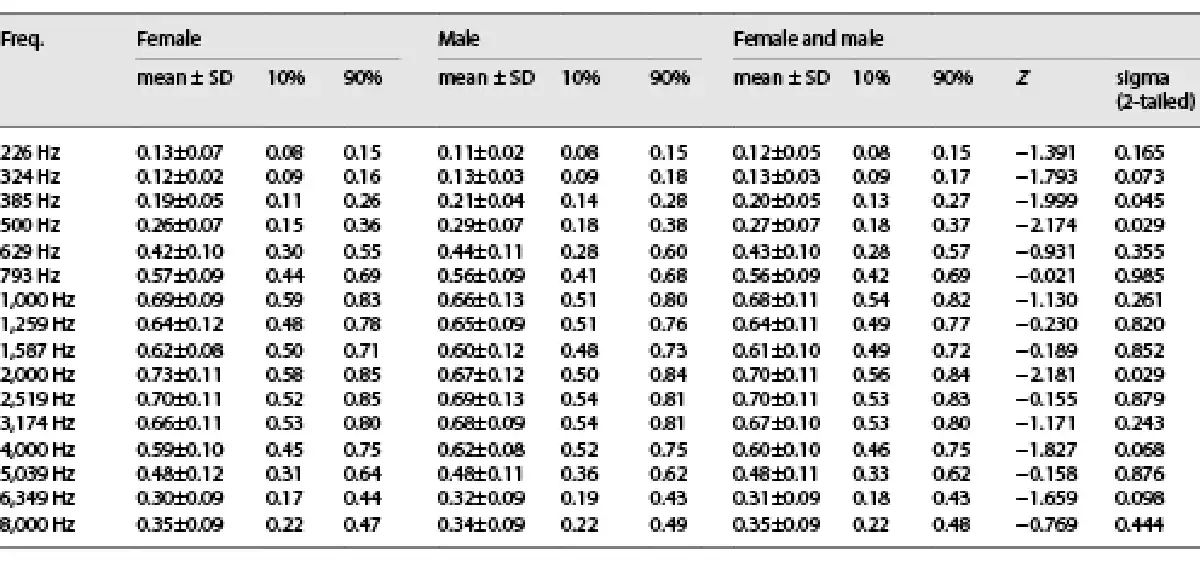
Table 4, shows the amount of EA values at different frequency levels in female and male subjects. Also, the means, standard deviations, and 10th and 90th percentiles, as well as the results from the Mann-Whitney U test have been presented in this table. Based on the statistical results released by the Mann-Whitney U test, there is a significant relationship between gender and EA at frequencies of 385 Hz, 500 Hz, and 2,000 Hz (p < 0.05, Table 4). Meanwhile, no statistical relationship was found between the EA and obtained frequencies.
Discussion
Norms have long been used as guidelines in evidence-based practice and can provide accurate judgment about the diagnosis. By having standard information about normal ranges, accurate measurements of the middle ear and hearing status can be tested. We provided a set of WBT data, collected from 101 (53 females and 48 males) Iranian adults with normal hearing and normal middle ear function that has been approved by the ENT physicians. It was ensured the subjects included in the study had normal hearing and middle ear function by taking precautions to minimize sampling bias. This study was intended to provide normative data for WBT of the young Iranian adult population and to provide information about influential factors such as ethnicity, gender, and age on it.
Ethnicity’s Impact on EA
Some studies have investigated differences in hearing sensitivity regarding the effects of ethnicity, gender, and aging on results of various audiological tests and their results such as Ad, ear canal volume, tympanometric width, and RF, etc. For instance, Shahnaz and Bork [2006] established that the Asian race has lower Ad, smaller ear canal volume, and wider tympanometric width compared to the Caucasian race. Moreover, multifrequency tympanometry studies showed that the Asian race has a higher RF than Caucasians [Shahnaz and Bork, 2006]. In the subsequent survey, they examined the EA in 128 adults aged 18–32 (62 Caucasians and 64 Chinese). They manifested that on low frequencies, the Chinese had lower EA than the Caucasian race, while the Caucasian race had a lower EA on higher frequencies. According to mentioned data, different norms should be procured for Caucasians and Chinese when assessing middle ear status by the WBT. Similarly, another study examined the amount of EA in Caucasian and Chinese people. This study has concluded that Chinese adults have lower EA below 1,250 Hz than those of Caucasian descent. However, the Caucasian race has a lower absorption rate at frequencies from 4,000 Hz to 6,000 Hz compared to the Chinese race. Furthermore, another population-specific study has been done in Turkey to evaluate the correlation between gender and EA values in Turkish ethnicity. The results of this research were as follows: among young Turkish adults (one hundred and ten participants) between 18 and 26 years old, the highest EA was at 2,519 and 3,174 Hz [Polat et al., 2015]. Regarding the results of our study, the highest value of EA in the Iranian race is 1,000, 2,000, and 2,519 Hz, which can be seen in Table 3 in both ears, respectively. One of the highest values of EA feature in WBT is 2,519 Hz as both investigations demonstrate in the Turkish and Iranian races.
In another similar article, the dynamic method (pressure sweep) was used in a descending manner from +250 to −300 daPa pressures in a study on 99 Caucasian Danish adults. In this manner, ear canal pressure decreases from +250 to −300 daPa at a pump speed of 100 daPa/s. Results of EA changes to pressure sweep mode along with the increment of frequencies from 256 to 1–2 kHz show a single peak. The quantity of EA increases with frequency, with the second peak occurring between 4 and 5 kHz; however, when frequency goes above 5 kHz, the amount of EA declines dramatically. EA rose from 0.18 to 0.71 from 256 to 1 kHz. There is a high closeness between the results of the present study and the study on the Danish Caucasian race. In both studies, the EA rate increases with increasing frequency, from 256 Hz to 1 kHz. While in our study, the EA rate decreases between frequencies 1 kHz and 2 kHz. In the mentioned paper, the EA rate is constant from 1 kHz to near 4 kHz. Both studies have reported an increase in the rate of EA at 8 kHz [Hougaard et al., 2020]. Kenny tested a total of 50 young adults (30 women, 20 men) at ambient pressure and dynamic (with introduced pressure changes) measures of wideband acoustic immittance in two equal ethnic groups (15 Chinese females, 10 Chinese males, 15 Caucasian females, and 10 Caucasian males). When comparing Caucasian and Chinese individuals in dynamic mode from 800 to 1,250 Hz, Kenny discovered that Caucasian subjects had much greater absorbance. Chinese respondents had considerably greater absorbance in the dynamic mode from 5,000 to 8,000 Hz than Caucasian subjects at higher frequencies [Kenny, 2011; Shahnaz et al., 2013].
Correlation among Tympanometry’s Features with Genders
Table 2 summarizes the tympanometric characteristics of participants of this study. In terms of RF, the difference between males and females was statistically significant (p > 0.05). In this study, females in the Iranian race had higher RF in both ears than males. In comparison to our findings, studies on frequency resonance and its association with gender have yielded inconsistent results. According to research done by Hunter and Margolis [1997] males showed significantly higher frequency resonance than females. Shahnaz and Davies [2006] observed no difference in RF between Caucasian and Chinese men and women in each group, despite the Chinese having a greater mean RF than their Caucasian counterparts. Some authors hypothesize that these variations in RF might be attributed to different Ad levels in males and females [Polat et al., 2015]. In addition, males had larger Veq than females and this notion can be manifested in this study too [Shahnaz and Davies, 2006]. TPP and G were measured in this study also. Table 2 shows that there were significant differences in TPP and G levels between the male and female groups (p > 0.05). This contradicts findings from previous research [Shahnaz and Davies, 2006]. Males and females showed a significant difference in terms of Ad between the two ears (p < 0.05). The Ad in the right and left ears are close together in both sexes, although males tend to have higher Ad. Likewise, Shahnaz and Davies [2006] conclude that Ad is higher in men than in women [Hougaard et al., 2020].
Gender’s Impact on WBT
One of the elements that might influence WBT is gender. Many investigations have been conducted in this field, but many various results have been obtained. Shahnaz et al. [2013] found that gender and frequency have a close relationship with EA rates. As a result, any alteration in frequency will affect the EA rate in both sexes. Females have higher absorbance than males at 4 kHz and 5 kHz [Shahnaz and Bork, 2006]. A very tight link between EA and gender was established in another thorough study done by Kenny on Caucasian and Chinese races to verify the relationship between gender and EA quantity with frequency variation. This research came in two modes: ambient pressure and TPP. In Ambient pressure, Chinese women showed higher EA levels at 4 kHz and 5 kHz than Chinese men, while there was no significant difference between men and women in the Caucasian race. But in TPP mode, EA at 5 kHz was higher in women than men [Kenny, 2011; Shahnaz et al., 2013]. In the Turkish population study stated earlier, a strong link between gender and EA was discovered in the frequency range of 3,100–6,900 Hz. Females showed greater absorption in high frequencies than males in this research [Polat et al., 2015]. We discovered a significant association (similarity) between gender and absorbance at 385 Hz, 500 Hz, and 2,000 Hz, with EA being greater in males at 500 Hz and 385 Hz and higher in women at 2,000 Hz. Shahnaz and Bork [2006] assumed that differences in body size of men and women are the probable reason for this. It should be added that in Hougaard’s study, they couldn’t find any association between EA and gender in the Danish Caucasian race. The lack of a significant influence of age and gender could be attributed to a participant variable that was not strictly controlled within the population sample and the fact that the study comprised a majority of women was considered the possible reason [Hougaard et al., 2020]. Mazlan emphasized in a survey with 101 adult participants (50 men and 51 women) conducted in 2015, that at lower frequencies, men had considerably more EA than women, but at higher frequencies, women had much higher EA [Mazlan et al., 2015].
Age’s Impact on WBT
One element that influences the amount of EA is age, however, it is worth noting that there are a few investigations in this field. Shahnaz and Bork [2006] found that in the frequency range of 2,500–5,000 Hz, adults of Caucasian and Chinese ethnicities had lower EA levels than school-aged children. Whereas in the Caucasian race, school-aged children have a lower amount of EA between 315 Hz and 1,250 Hz than young adults. This difference is probably due to differences in body size and subsequently middle ear size [Shahnaz and Bork, 2006]. The middle ear and the TM properties alter as we become older. They had greater EA rates at frequencies below the maximum EA level and lower EA rates at frequencies above the maximum absorption rate than young adults [Sanford and Feeney, 2008]. Analogous to Shahnaz and Bork, Beers et al. [2010] tried to obtain normative data for school-aged children with a mean age of 6.15 years, ranging from 5 years and 1 month to 6 years and 11 months, in Caucasian (63 ears), Chinese (60 ears), and mixed (21 ears) ethnicity. The highest mean EA value for the Caucasian group is about 3,492 Hz, whereas the highest mean EA value for the Chinese group is around 2,367 Hz [Beers et al., 2010]. Mazlan perused the influence of age of EA in 40 young adults (14 men, 26 women, aged 20–38 years), 31 middle-aged adults (16 men, 15 women, aged 42–64 years), and 30 older adults (20 men, 10 women, aged 65–82 years) precisely. The young adult group exhibited much lower EA (between 400 and 560 Hz) than the middle-aged group, according to the findings. The middle-aged group, on the other hand, had a much lower EA than the young adult group (between 2,240 and 5,040 Hz). Furthermore, the EA of older adults was much lower than that of young adults (between 2,520 and 5,040 Hz). There was no significant difference in EA between middle-aged and older persons at any frequency [Mazlan et al., 2015].
Conclusion
WBT is one of the new methods to evaluate the status of the middle ear with high sensitivity and vitality compared to conventional tympanometry. However, the use of this method is not currently common in clinical evaluations. Many researchers have tried to obtain normative data, which is a standardized criterion for any evaluation, and have obtained relevant information according to the structural characteristics of ears of each race. This study aimed to obtain normative data for young Iranian adults and the difference between male and females in terms of WBT were investigated. 101 Iranian adults (53 males and 48 females) aged 19–29 years were evaluated with normal hearing and normal 226-Hz tympanometry. In the Iranian race, the highest rate of EA is at frequencies of 1,000 Hz, 2,000 Hz, and 8,000 Hz. There is conflicting information about various factors affecting EA rates at different frequencies, such as the impact of gender and age. In this study, the effect of gender on EA was evaluated and according to statistical analysis, there was a significant relationship (p ≤ 0.05) between gender and EA level at 385 Hz, 500 Hz, and 2,000 Hz. According to these results, it can be concluded that using separate norms for males and females may increase test specificity and sensitivity. It can be concluded that different norms for male and female young adults may have a diagnostic value. Normative data for WBT are limited, and this study aimed to obtain normative data to facilitate the diagnosis of various middle ear diseases, especially otosclerosis and middle ear infection.
Acknowledgments
This study was conducted to improve the diagnosis of ENT-related diseases and to increase the use of WBT for correct diagnosis. We are grateful to all the participants who took part in this study voluntarily. The relationship between acoustic reflex and race would be a novel subject for future studies.
Statement of Ethics
This study was carried out in strict accordance with the recommendations of the Nursing, Rehabilitation and Management Schools-Isfahan University of Medical Science’s subcategory of the Iranian National Committee for Ethics in Biomedical Research by approval number of IR.MUI.RESEARCH.REC.1397.193. All the volunteers taking part in this clinical study have received verbal and written information and have been able to ask questions about the study. They willingly signed an informed consent form before starting the tests.
Conflict of Interest Statement
The authors have no conflicts of interest to declare.
Funding Sources
The research represents the authors’ work, without external funding.
Author Contributions
Mohammad Hossein Nilforoush and Mahsa Sepehrnejad have conceived and designed the idea of this studying. Zahra Habibi is the responsible author for gathering information and statistical analyses. Farshid Rahimi wrote the manuscript. All the authors provided significant inputs to the first version of the manuscript. All the authors read and approved the final version of the manuscript.
Data Availability Statement
All data that had been gathered or analyzed during this study are included in this article. Further inquiries can be directed to the corresponding author that will be sent to Editorial Office if required anytime.
References
- 1. Aithal S, Kei J, Driscoll C, Khan A, Swanston A. Wideband absorbance outcomes in newborns: a comparison with high-frequency tympanometry, automated brainstem response, and transient evoked and distortion product otoacoustic emissions. Ear Hear. 2015;36(5):e237–50. https://doi.org/10.1097/AUD.0000000000000175.
- 2. Alaerts J, Luts H, Wouters J. Evaluation of middle ear function in young children: clinical guidelines for the use of 226-and 1,000-Hz tympanometry. Am J Otol. 2007;28(6):727–32. https://doi.org/10.1097/mao.0b013e3180dca1e5.
- 4. André KD, Sanches SGG, Carvallo RMM. Middle ear resonance in infants: age effects. Int Arch Otorhinolaryngol. 2012;16(3):353–7. https://doi.org/10.7162/S1809-97772012000300009.
- 5. Baldwin M. Choice of probe tone and classification of trace patterns in tympanometry undertaken in early infancy: Selección de la sonda de prueba y clasificación de la curva de timpanometría en la infancia temprana. Int J Audiol. 2006;45(7):417–27. https://doi.org/10.1080/14992020600690951.
- 6. Beers AN, Shahnaz N, Westerberg BD, Kozak FK. Wideband reflectance in normal Caucasian and Chinese school-aged children and in children with otitis media with effusion. Ear Hear. 2010;31(2):221–33. https://doi.org/10.1097/AUD.0b013e3181c00eae.
- 7. Camboim ED, Scharlach RC, Almeida MCO, Vasconcelos D, Azevedo MF. Análise da compliância e gradiente timpanométrico em lactentes com refluxo. Rev Soc Bras. 2012;17(2):156–60. https://doi.org/10.1590/s1516-80342012000200009.
- 8. Feeney MP, Keefe DH, Hunter LL, Fitzpatrick DF, Garinis AC, Putterman DB, et al. Normative wideband reflectance, equivalent admittance at the tympanic membrane, and acoustic stapedius reflex threshold in adults. Ear Hear. 2017;38(3):e142–60. https://doi.org/10.1097/AUD.0000000000000399.
- 9. Feeney MP, Grant IL, Marryott LP. Wideband energy reflectance measurements in adults with middle-ear disorders. J Speech Lang Hear Res. 2003;46(4):901–11. https://doi.org/10.1044/1092-4388(2003/070).
- 10. Feeney MP, Stover B, Keefe DH, Garinis AC, Day JE, Seixas N. Sources of variability in wideband energy reflectance measurements in adults. J Am Acad Audiol. 2014;25(5):449–61. https://doi.org/10.3766/jaaa.25.5.4.
- 11. Hoffmann A, Deuster D, Rosslau K, Knief A, am Zehnhoff-Dinnesen A, Schmidt C-M. Feasibility of 1000 Hz tympanometry in infants: tympanometric trace classification and choice of probe tone in relation to age. Int J Pediatr Otorhinolaryngol. 2013;77(7):1198–203. https://doi.org/10.1016/j.ijporl.2013.05.001.
- 12. Hougaard DD, Lyhne NM, Skals RK, Kristensen M. Study on wideband tympanometry and absorbance within a Danish cohort of normal hearing adults. Eur Arch Otorhinolaryngol. 2020;277(7):1899–905. https://doi.org/10.1007/s00405-020-05909-9.
- 13. Hunter LL, Margolis RH. Multifrequency tympanometry: current clinical application. Am J Audiol. 1992;1(3):33–43.
- 14. Hunter LL, Margolis RH. Effects of tympanic membrane abnormalities on auditory function. J Am Acad Audiol. 1997;8(6):431–46.
- 15. Kei J, Allison-Levick J, Dockray J, Harrys R, Kirkegard C, Wong J, et al. High-frequency (1000 Hz) tympanometry in normal neonates. J Am Acad Audiol. 2003;14(1):20–8. https://doi.org/10.3766/jaaa.14.1.4.
- 17. Lilly DJ, Margolis RH. Wideband acoustic immittance measurements of the middle ear: introduction and some historical antecedents. Ear Hear. 2013;34(Suppl 1):4s–8s. https://doi.org/10.1097/AUD.0b013e31829db80f.
- 18. Mazlan R, Kei J, Ya CL, Yusof WNHM, Saim L, Zhao F. Age and gender effects on wideband absorbance in adults with normal outer and middle ear function. J Speech Lang Hear Res. 2015;58(4):1377–86. https://doi.org/10.1044/2015_JSLHR-H-14-0199.
- 19. Noh H, Lee D-H. Direct measurement of ear canal volume in a pediatric population: can we explain its individual variation in terms of age and body weight?Int J Pediatr Otorhinolaryngol. 2012;76(5):658–62. https://doi.org/10.1016/j.ijporl.2012.01.035.
- 20. Onusko EM. Tympanometry. Am Fam Physician. 2004;70(9):1713–20.
- 21. Özgür A, Müjdeci B, Terzi S, Özergin Coşkun Z, Yigit E, Dursun E. Wideband tympanometry normative data for different age groups in Turkish population. J Int Adv Otol. 2016;12(1):82–6. https://doi.org/10.5152/iao.2015.1408.
- 22. Polat Z, Baş B, Hayır D, Bulut E, Ataş A. Wideband tympanometry normative data for Turkish young adult population. J Int Adv Otol. 2015;11(2):157–62. https://doi.org/10.5152/iao.2015.809.
- 23. Sanford CA, Brockett JE. Characteristics of wideband acoustic immittance in patients with middle-ear dysfunction. J Am Acad Audiol. 2014;25(5):425–40. https://doi.org/10.3766/jaaa.25.5.2.
- 24. Sanford CA, Hunter LL, Feeney MP, Nakajima HH. Wideband acoustic immittance: tympanometric measures. Ear Hear. 2013;34(Suppl 1):65s–71s. https://doi.org/10.1097/AUD.0b013e31829c7250.
- 25. Sanford CA, Feeney MP. Effects of maturation on tympanometric wideband acoustic transfer functions in human infants. J Acoust Soc Am. 2008;124(4):2106–22. https://doi.org/10.1121/1.2967864.
- 26. Shahnaz N, Bork K. Wideband reflectance norms for Caucasian and Chinese young adults. Ear Hear. 2006;27(6):774–88. https://doi.org/10.1097/01.aud.0000240568.00816.4a.
- 27. Shahnaz N, Davies D. Standard and multifrequency tympanometric norms for Caucasian and Chinese young adults. Ear Hear. 2006;27(1):75–90. https://doi.org/10.1097/01.aud.0000194516.18632.d2.
- 28. Shahnaz N, Feeney MP, Schairer KS. Wideband acoustic immittance normative data: ethnicity, gender, aging, and instrumentation. Ear Hear. 2013;34(Suppl 1):27s–35s. https://doi.org/10.1097/AUD.0b013e31829d5328.
- 29. Shahnaz N, Bork K. Comparison of standard and multi-frequency measures obtained with the virtual 310 system and the Grason-Stadler Tympstar. Can J Speech-Lang Pathol Audiol. 2008;32(4):146–57.
- 30. Shurin PA, Pelton SI, Finkelstein J. Tympanometry in the diagnosis of middle-ear effusion. N Engl J Med. 1977;296(8):412–7. https://doi.org/10.1056/NEJM197702242960802.
- 3. American Academy of Family Physicians; American Academy of Otolaryngology-Head and Neck Surgery; American Academy of Pediatrics Subcommittee on Otitis Media With Effusion. Otitis media with effusion. Pediatrics. 2004; 113(5): 1412–29.
- 16. Kenny SPVN. Clinical application of the Interacoustics REFLWIN system wideband reflectance machine in the assessment of the eustachian tube. University of British Columbia. 2011. Retrieved from https://open.library.ubc.ca/collections/ubctheses/24/items/1.0072303.