The integral role of cardiac imaging in cardiology
Non-invasive and invasive imaging of the heart is central to diagnosis, risk assessment, therapeutic decision-making, medical and invasive therapies, prognosis, and long-term monitoring in Cardiology. Cardiac imaging is thus central in striving for precision medicine, the essence of which is the provision of individualized care to each and every patient. Examples of such imaging performed by cardiologists include: (i) invasive coronary angiography and cardiac computed tomography (CCT); (ii) cardiovascular magnetic resonance (CMR); (iii) echocardiography; (iv) nuclear cardiology; and (v) advanced invasive imaging (optical coherence tomography and intracardiac echocardiography). For all these imaging modalities we highlight the importance of an in-depth understanding of cardiovascular pathology, complex physiology, and the consequences of imaging findings in the management of cardiovascular health and disease.
Cardiologists and cardiac imaging core competencies
Imaging is a core competency of all cardiologists, with echocardiography and coronary angiography (both invasive and non-invasive) an important aspect of training and firmly embedded in mainstream cardiology practice. In the core cardiology curriculum applicable to all cardiologists, the European Association of Cardiovascular Imaging (EACVI) was integral to the development of all imaging capabilities and standards which are used to train cardiologists who are then formally assessed by the European Examination in Core Cardiology.
Cardiologists consider disease process, pathology, and management options rather than purely the individual imaging modality, placing them in a unique position to select the most appropriate imaging test for each specific clinical scenario, taking patient preference into account.
Imaging expertise alone is not sufficient for patient management
Accurate, efficient, and effective cardiac imaging requires not only intricate knowledge of imaging modalities, and the adaptations that are required to optimize imaging protocols to the physiological condition of each individual patient, but also of the rapidly changing field of cardiovascular medicine.
For decades, cardiologists have independently performed invasive and non-invasive imaging modalities from ultrasound (transthoracic and transoesophageal echocardiography) to x-ray-based angiography (invasive cardiac and coronary angiography and intervention), which has significantly contributed to the improved management of cardiovascular diseases and outcomes. Cardiologists are uniquely placed to naturally integrate into their clinical practice computed tomography (CT) and CMR which complement their existing anatomical (invasive angiography) and functional (echocardiography) imaging tests.
Translational research in cardiac imaging leading to a paradigm shift in cardiovascular clinical practice has been driven predominantly by cardiologists including roles in image interpretation and quality control in core labs, and participation in commercial trials. Examples of investigator-led research relevant to chronic coronary syndromes include the ISCHEMIA trial, the SCOT-HEART trial, the MR-INFORM trial, and the DISCHARGE trial. The results of these trials have transformed cardiovascular medicine practice within the last years.
The portfolio of up-to-date clinical practice guidelines and clinical consensus statements for the diagnosis and management of cardiovascular disease published by the European Society of Cardiology (ESC) and EACVI are used by millions of practitioners worldwide. These documents, written by cardiovascular practitioners for cardiovascular practitioners, include recommendations on which cardiac imaging modality to choose, what to expect from the report, and how to act on relevant findings. Cardiologists are fully trained and competent to produce information for patients undergoing the examination and preparation involved, to supervise patients’ preparation on the day of the test, and to consent patients to the test (including stress tests and CMR in patients with cardiac devices). Imaging cardiologists are trained in image acquisition, image post-processing and reconstruction, and image interpretation. Thanks to their in-depth knowledge of cardiovascular physiology and pathology, cardiologists are uniquely positioned to produce a clinically meaningful cardiac imaging report with adequate description and interpretation of the findings that the referring physician (cardiologists in most cases) can act upon. Cardiologists reporting imaging are also well-positioned to provide clinical advice on further additional testing (e.g. genetic testing or myocardial biopsy) or initiation of therapy (such as revascularization or cardiac device implantation).
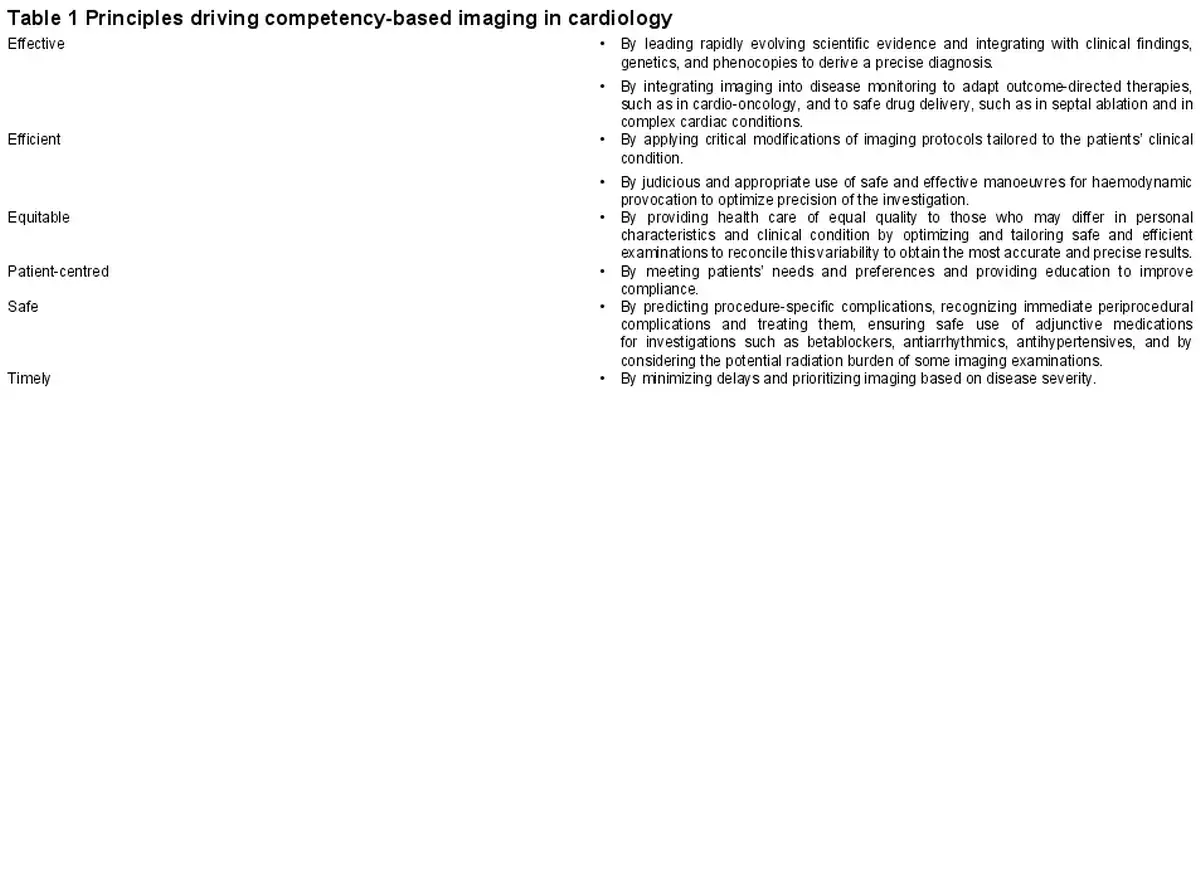
Similarly, the treatment of patients with structural heart disease continues to expand cardiology practice. Structural heart interventions depend on imaging which is central to pre-, peri-, and post-procedural management to balance procedural risk and appropriate patient selection. Importantly, imaging and imaging results must often be immediately available (e.g. in the context of complications) or are integrated into the procedure itself. Without this in-depth knowledge of the fast-changing field of cardiovascular medicine, even expert cardiac imagers would not provide the highest quality services. The core principles of competency are effectiveness, efficiency, equity, patient-centredness, safety, and timeliness (Table 1). They apply to all imaging modalities. They need to be adapted to each individual patient to be safe and effective, with particular attention to patient heart rate and rhythm in order to be safe, which is key for the delivery of value-based cardiac imaging. Examples include exercise or pharmacologically induced stress imaging (echocardiography, CMR, nuclear cardiology, CT perfusion), ensuring low radiation exposure and high image quality using beta-blockers for CCT, emergency indications for cardiac imaging, such as suspected pulmonary embolism, aortic dissection, acute and severe mitral valve regurgitation after myocardial infarction.
Cardiologists can also capitalize on their intricate knowledge and experience in cardiovascular pharmacology, from the prescription and administration of beta-blockers, vasodilator stress agents, including indication and contraindications on the use of these drugs during cardiac imaging tests, as well as extensive experience in advanced life support in case of cardiac and respiratory arrest, thus significantly improving patients’ safety. Many cardiology imaging services and the imaging training offered are dependent on cardiologists and have been developed by cardiologists, either in conjunction with other specialties (such as radiology) or as stand-alone departments.
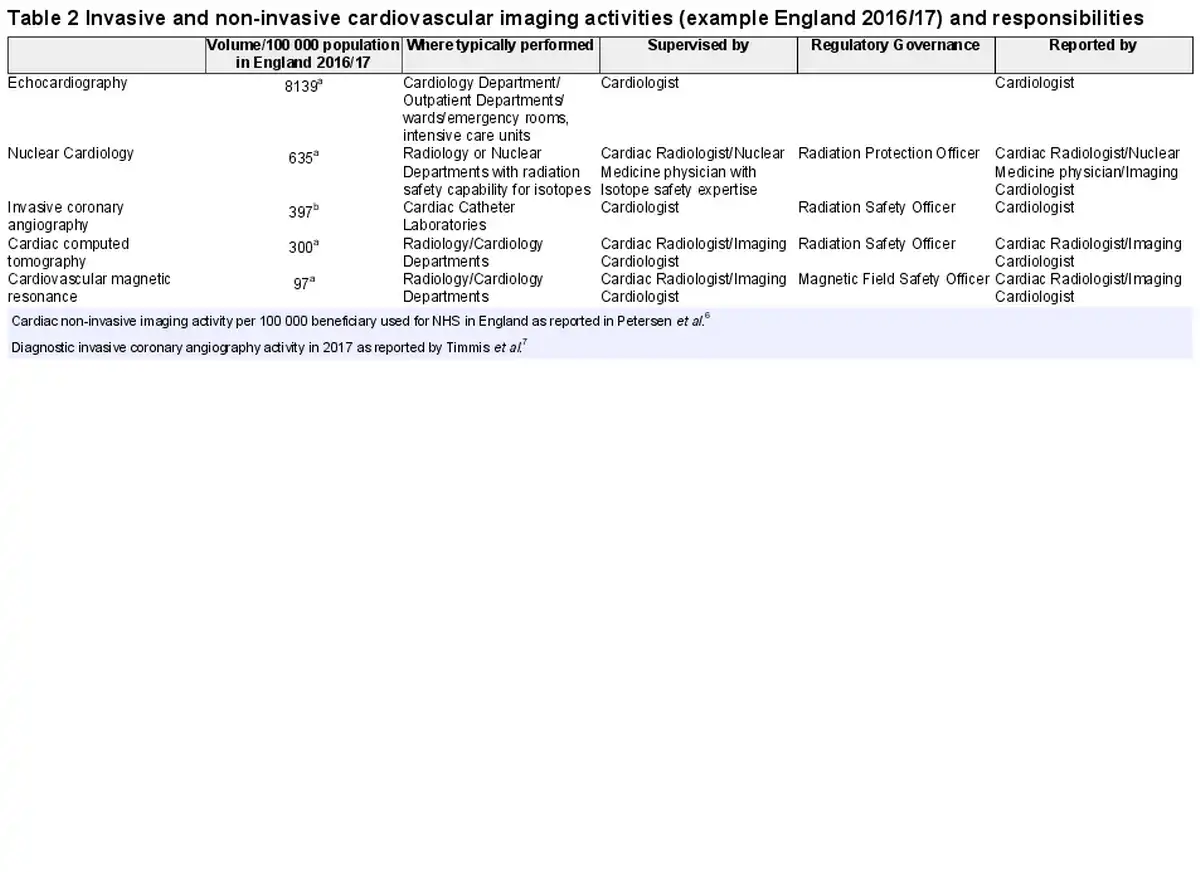
The demand for cardiac imaging is increasing (Figure 1) and in many countries, there is a need to train more individuals to provide high-quality cardiac imaging services to meet this demand. The combination of imaging and cardiology expertise is essential not only for the optimal application of imaging tests but also for the appropriate interpretation of cardiac imaging findings. Echocardiography is the most frequently performed cardiac imaging test (Table 2) and is firmly embedded within cardiology services independent of service size, scope (hospitals for secondary, tertiary, or quaternary care), and setting (inpatient/outpatient). Furthermore, this makes echocardiography practical in many settings such as rapid assessment of response to treatments, screening of family members, and general assessment of the patients’ overall cardiological condition. Cardiology is both central and integral to cardiac imaging, and while collaboration with cardiac radiologists and nuclear cardiology physicians can be useful and is encouraged, it is not essential as long as the required expertise is covered by the imaging cardiologist, which is often the case (Table 2). Many highly successful Cardiology-led departments have been established with reputations for national and international excellence. Where services are conjoint between experts, there is evidence that this both enhances the quality of care and leads to rapid service growth, such as that seen in CCT in the United States of America.
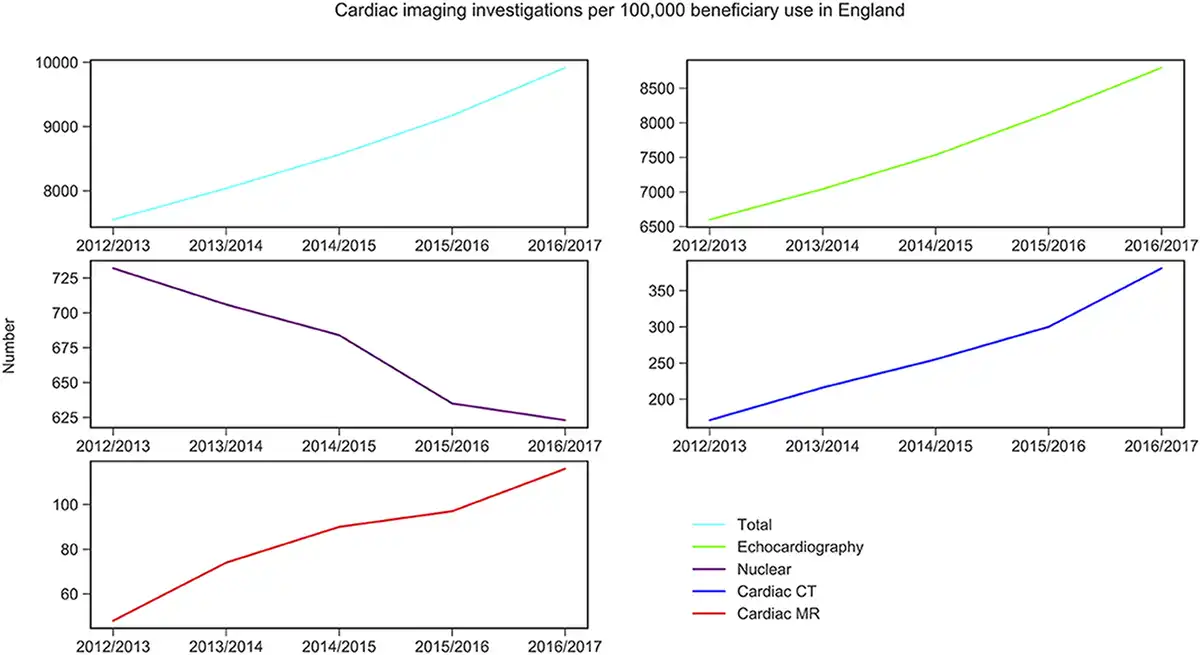
Figure 1
Increasing demand for non-invasive cardiovascular imaging as illustrated for England. Data are challenging to collect across Europe, but trends would be expected to be similar in many European countries. From Petersen et al.
EACVI certification programme to deliver high quality and equal access to patient care
To define the scope of practice of clinicians across non-invasive cardiac imaging modalities there is a series of complementary and integrated curricula and syllabi developed by the EACVI for advanced training in each specific modality. Commencing in 2003 with a single examination for transthoracic echocardiography, the EACVI certification programme now encompasses all four imaging modalities with seven dedicated certification programmes (three for echocardiography, two for CMR, one for CCT, and one for nuclear cardiology). There has been a steady, consistent year-on-year increase in uptake of these programmes with currently over 1000 candidates annually (Figure 2).
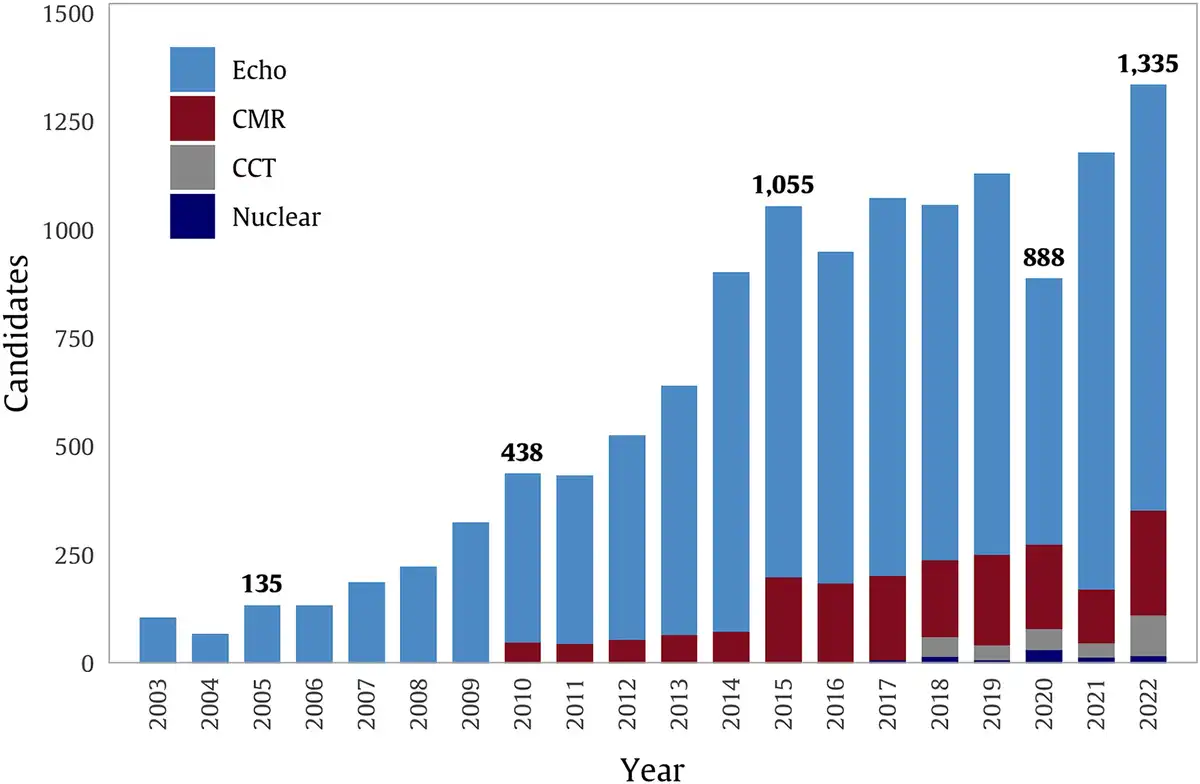
Figure 2
The certification offerings by the European Association of Cardiovascular Imaging have broadened over the last 20 years across four imaging modalities. CCT, cardiac computed tomography; CMR, cardiovascular magnetic resonance; Echo, echocardiography; Nuclear, nuclear cardiology. Uptake shows increasing trends now well above one thousand individual certifications per year.
Each certification programme has a specific examination which has evolved over time. From handwritten examinations which were manually marked and graded, these examinations now use a multiple-choice format with well-documented methodology for standard setting and determination of pass marks and pass rates. The examination delivery method has also evolved to a computer-based examination with remote proctoring allowing candidates to take these examinations from any location. This has increased the numbers of candidates but critically maintains examination security. This also maintains consistency with the ESC core cardiology examination with increasing numbers of candidates (Figure 3). It includes a published blueprint, weighting the key components of the curriculum for the examination, question writing and standard-setting groups, and consistent methodology for pass mark determination. The full examination cycle for each of the EACVI examinations replicates the process used for the ESC European Examination in Core Cardiology.
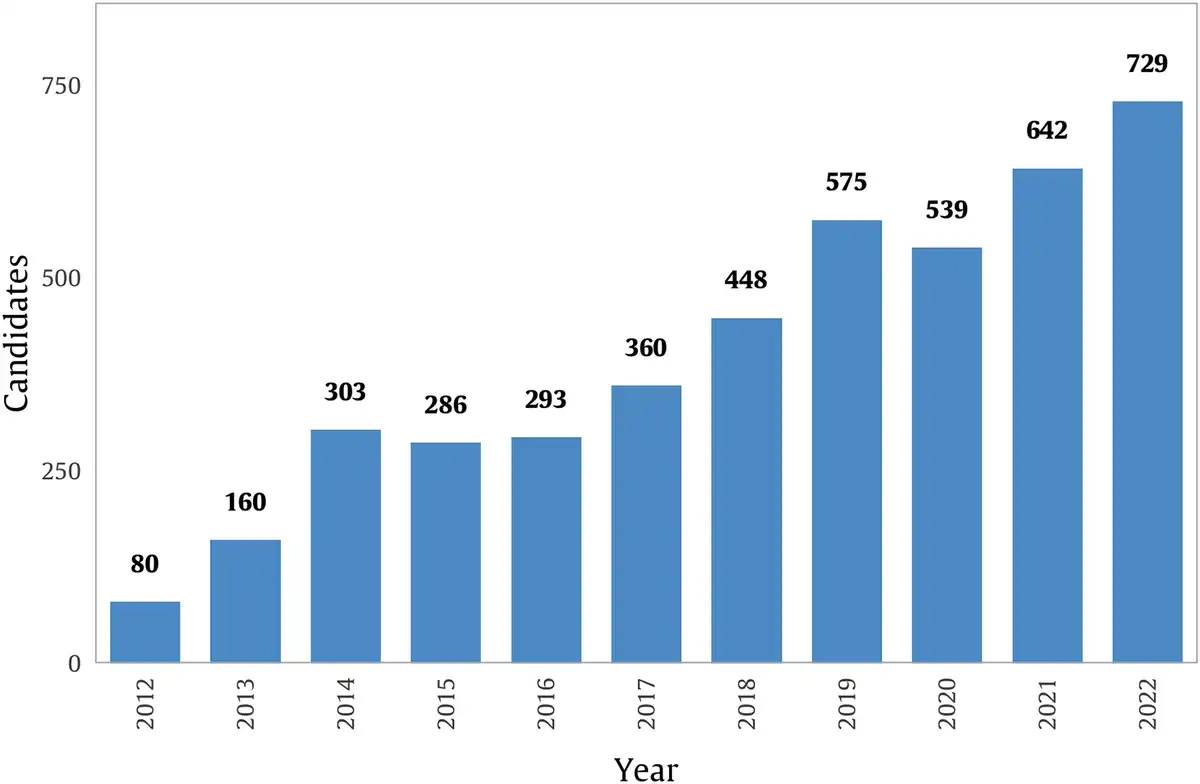
Figure 3
Increasing numbers of candidates taking the European Society of Cardiology core cardiology examination. This examination ensures cardiologists know when and how cardiac imaging can help their patient management (level 1).
With several modalities, there are different levels of certification. The basic level of education is established in level I and focuses on the clinical indications and basic knowledge of the technique and appropriate use following the guidelines of each cardiovascular disease. Level I courses at conferences or local initiatives are secured through central endorsement by the EACVI/ESC and supported throughout Europe and beyond. Also, EACVI has provided a certified online level I course for each of the four modalities since 2022. The advanced levels of certification, levels II and III, further elaborate on theoretical knowledge, but also largely consist of practical education. Level II emphasizes competency to acquire images (including technical considerations), interpret these images, and provide a structured report of salient findings. It is defined as the minimum standard to report independently (Figure 4). Level III requires a wider and more in-depth understanding of the modality including publications and evidence of training others (Figure 5). It also includes other aspects of delivering a full cardiac imaging service. Important parts of the full service include data handling and secure storage, patient safety (particularly for CMR, CCT, and nuclear cardiology), and liaison with the multi-professional team (such as the ability to present cases at a multidisciplinary meeting). This is furthermore true in the acute and emergency setting where collaboration with critical care and emergency medicine colleagues is common practice. The volume of reported cases required is also higher. In line with evolving trends, online case repositories or cases reviewed during didactic teaching can also be submitted in part as evidence recognizing a move to more online education. In case there is no certified professional in the trainees’ hospital, remote teaching is arranged to supervise the expansion of knowledge and competence.
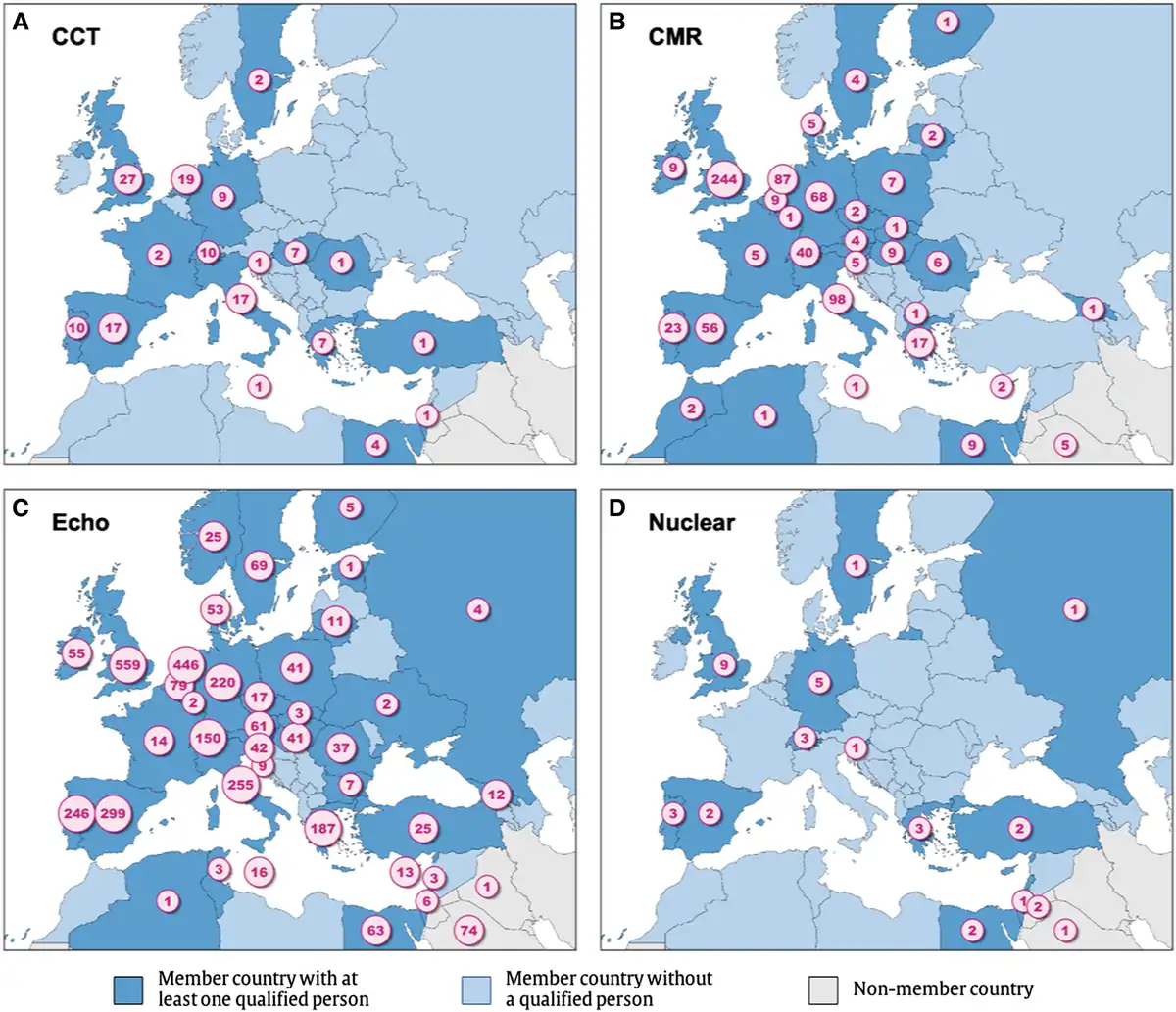
Figure 4
Number of levels 2 or 3 certified individuals across the four imaging modalities. CCT, cardiac computed tomography; CMR, cardiovascular magnetic resonance; Echo, echocardiography; Nuclear, nuclear cardiology. Levels 2 or 3 certification indicates individuals that have the competency to be part of an imaging service and provide and sign-off imaging reports independently. As CCT and Nuclear certification programmes are recent, there is a gap between expert reporters and having obtained certification—this gap is likely to close over the coming few years (data are shown as of 26 March 2023).
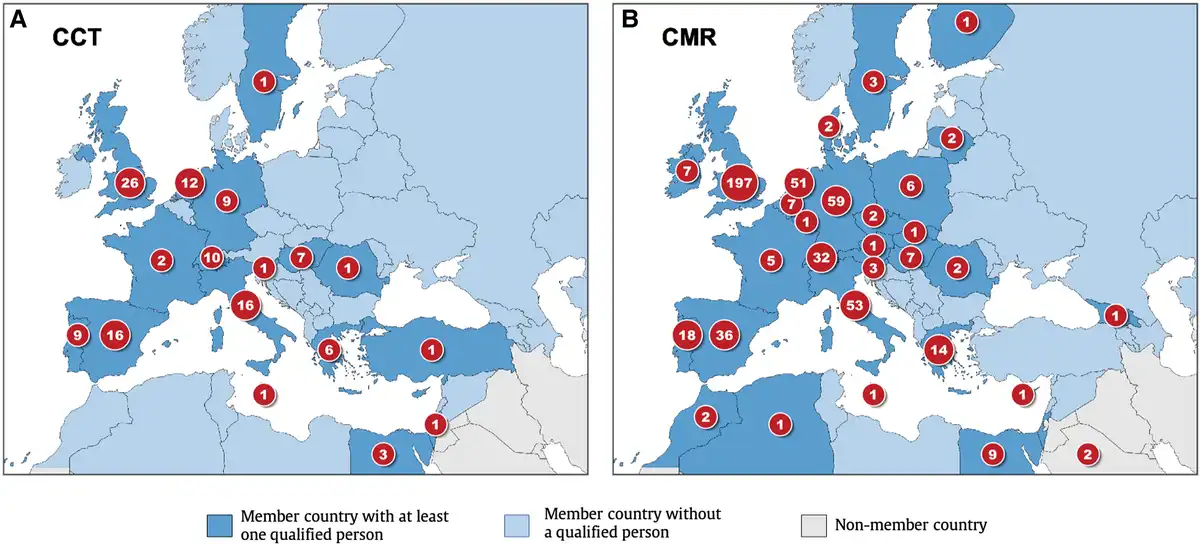
Figure 5
Number of level 3 certified individuals across imaging modalities. CCT, cardiac computed tomography; CMR, cardiovascular magnetic resonance. Level 3 certification indicates qualification and standards to be able to train the next generation of levels 2 and 3 certified physicians. Granular level data were not available for echo or nuclear modalities. Some countries do not have a level 3 certified individual, and the European Association of Cardiovascular Imaging is exploring ways of supporting the expansion of level 3 certified physicians to more countries. Data shown as of 26 March 2023.
To implement standardization in education and to provide valuable official output for practitioners, scientists, policymakers, and the public, EACVI also publishes several official documents each year, including recommendation papers, consensus statements, and position statements, which follow a thorough methodology and an extensive review process. While a patient-centred approach leads to the creation of multi-modality imaging recommendations, focus is also given to each distinct modality governed by the EACVI.
EACVI integrated training programme
At all levels, the need to integrate imaging is central to the entire programme of certification. This is not simply ensuring the optimal use of limited resources for cardiac diagnostic testing but also relates to the training of future cardiologists, integration with colleagues across the multi-professional team, and the focus on patient-centred care. The use of cardiac pathology to drive the overall shape and construction of each curriculum ensures consistency with the core cardiology curriculum (as opposed to a more modality-centred curriculum) and allows a trainee seamlessly to build on the core knowledge in each modality already attained. It facilitates concomitant training in multiple modalities, stressing the use of pathophysiology and disease processes to determine the optimal use of investigations and avoiding layered, multiple, and duplicate testing. Integration of cardiac imaging in the overall investigation and management of patients maintains the most patient-focused care. In more complex cases this approach cements the role of case discussion across the multi-professional team at clinical case conferences or multidisciplinary team meetings.
To further recognize the role of integrated multi-modality imaging the ESC is supporting a shift towards multi-modality imaging congresses with EACVI 2023 being the first such multi-modality congress. In May 2023 EACVI launched a multi-modality certification and continues this trend. Though initially, this will simply recognize an individual certified in two complementary imaging modalities this will evolve further in the future with the ever-increasing emphasis on disease and patient-focused care placing the emphasis on the imaging specialist with an in-depth understanding of all imaging modalities but a high level of expertise in two or more of them.
A new perspective on competency-based cardiac imaging supported by patients
A recent report by the European Society of Cardiovascular Radiology and European Society of Radiology on the status and vision of cardiac radiology in Europe emphasizes the need to increase cardiac imaging expertise and capacity amongst radiologists. This report, however, fails to acknowledge the integral nature of cardiologists in cardiac imaging. We strongly disagree with the implied perspective that radiology alone is critical and always required for cardiac imaging and thus we do not endorse the content of this report. Furthermore, as already stated, there are multiple world-renowned imaging departments that are wholly Cardiology led, directed, and managed from inception and which continue to deliver cutting-edge clinical services, training, and academic outputs.
Cardiac imaging has evolved to become central to cardiovascular disease management and imaging investigations are frequently amongst the first investigations requested by clinicians. The central and expanding role of cardiac imaging to identify and risk stratify pathology and guide treatment will continue to evolve and develop in the coming years. Using a clearly defined competency framework these cardiac imaging standards equip cardiologists with the necessary expertise but can apply equally to all medical specialists, irrespective of previous experience, training, and specialty.
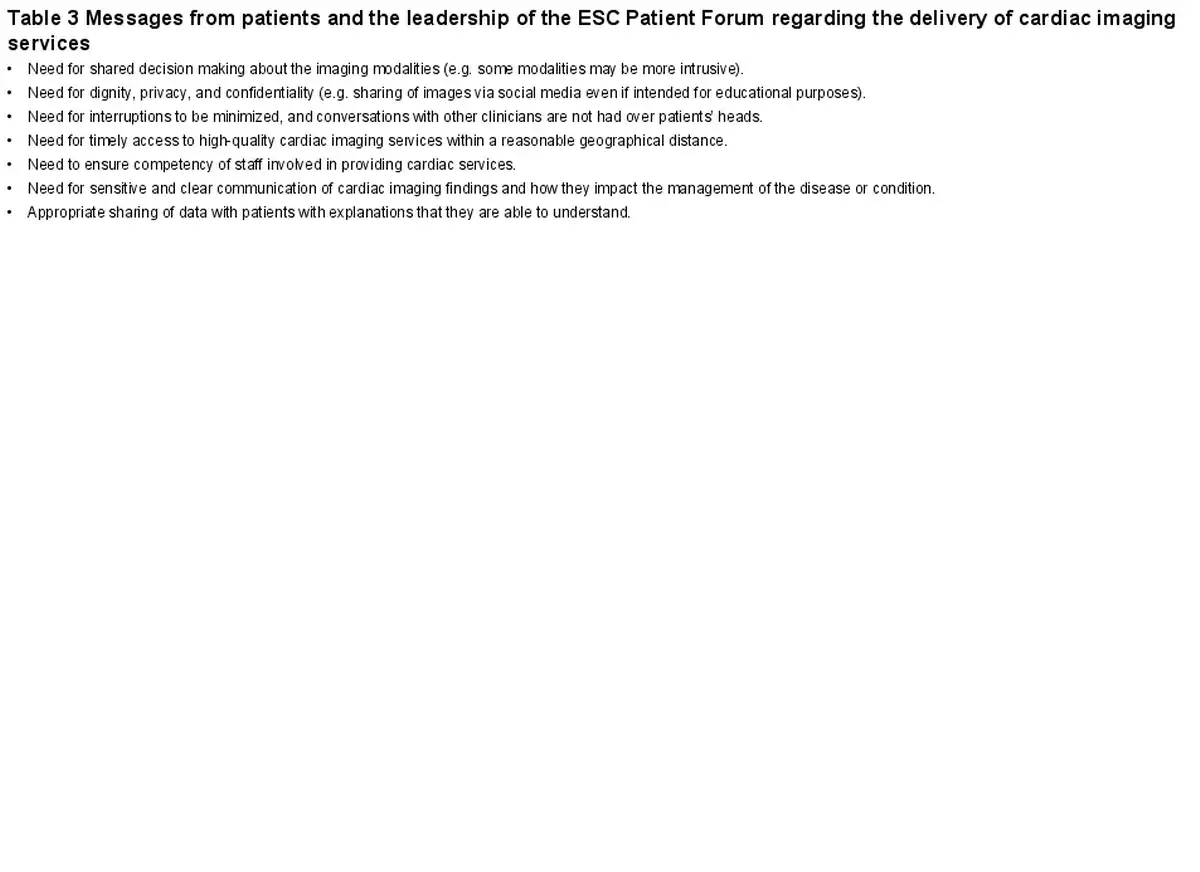
Finally, and importantly, the ultimate voice is that of our patient. In discussion with patients and the leadership of the ESC Patient Forum, we captured key statements related to cardiac imaging (Table 3). Patients assign little importance to which modality or which speciality (cardiology, radiology, nuclear medicine, and critical care) provides the investigations. Patients just want to receive the best care possible. In the future, this will become more important as we use imaging to directly guide treatment and therapeutic decision making.
Digital innovations and competency-based cardiac imaging
Human experts and cardiac imaging competency will continue to be indispensable in the future, despite a fast-changing landscape impacting cardiac imaging with innovations in digital health and artificial intelligence (AI). First, the development and iterative improvement of AI solutions in cardiac imaging using supervised learning requires expert image annotations. Second, human expert assessment of AI-enabled cardiac image segmentations will require competency. Undoubtedly, we will see many changes in cardiac imaging through digital innovation, but human competency will work hand in hand with AI-enabled solutions to provide better care to patients.
Conclusions
Imaging is integral to Cardiology. There is a major demand to increase capacity in expert cardiac imaging services and the frameworks devised, developed, and implemented by the ESC and EACVI equip cardiologists to provide these services. EACVI promotes collaborative approaches to cardiac imaging between specialties where possible and desired. The main mission of EACVI is to promote and spread the appropriate use of cardiac imaging throughout all member countries. A professional barrier created around ‘specialty-based’ rather than ‘competence-based’ delivery of cardiac services (in particular for CCT and CMR) has been one of the major limiting factors for the wider use of fundamental diagnostic tests in many countries. To foster the efficient and effective use of cardiac imaging in modern cardiology, in some countries, legislation governing who can deliver imaging may need to be revisited. EACVI and the ESC support a competency-based cardiac imaging service delivery that will assure availability and optimal quality for the benefit of our patients (Table 4 and Graphical Abstract).
Acknowledgements
This paper was developed by the European Society of Cardiology with special contribution from the European Association of Cardiovascular Imaging (EACVI) and was then endorsed by the European Society of Cardiology Associations: the Association of Cardiovascular Nursing & Allied Professions (ACNAP), the Association for Acute CardioVascular Care (ACVC), the European Association of Preventive Cardiology (EAPC), the European Association of Percutaneous Cardiovascular Interventions (EAPCI), the European Heart Rhythm Association (EHRA), and the Heart Failure Association (HFA). The document was reviewed by the European Association of Cardiovascular Imaging (EACVI) Board and approved by the ESC Scientific Documents Committee. We are grateful to Celeste McCracken for her help in creating the figures containing certification data; Liliana Szabo for her help in creating the graphical abstract; and Matthieu Depuydt (European Society of Cardiology) for coordination support to the manuscript development.
References
- 1. Cuocolo R, Ponsiglione A, Dell'Aversana S, D'Acierno L, Lassandro G, Ugga L, et al The cardiac conundrum: a systematic review and bibliometric analysis of authorship in cardiac magnetic resonance imaging studies. Insights Imaging2020;11:42. https://doi.org/10.1186/s13244-020-00850-1
- 2. Maron DJ, Hochman JS, Reynolds HR, Bangalore S, O'Brien SM, Boden WE, et al Initial invasive or conservative strategy for stable coronary disease. N Engl J Med2020;382:1395–407. https://doi.org/10.1056/NEJMoa1915922
- 3. Newby DE, Adamson PD, Berry C, Boon NA, Dweck MR, et alSCOT-HEART Investigators Coronary CT angiography and 5-year risk of myocardial infarction. N Engl J Med2018;379:924–33. https://doi.org/10.1056/NEJMoa1805971
- 4. Nagel E, Greenwood JP, McCann GP, Bettencourt N, Shah AM, Hussain ST, et al Magnetic resonance perfusion or fractional flow reserve in coronary disease. N Engl J Med2019;380:2418–28. https://doi.org/10.1056/NEJMoa1716734
- 5. Maurovich-Horvat P, Bosserdt M, Kofoed KF, Rieckmann N, Benedek T, et alDISCHARGE Trial Group CT Or invasive coronary angiography in stable chest pain. N Engl J Med2022;386:1591–602. https://doi.org/10.1056/NEJMoa2200963
- 6. Petersen SE, Friebel R, Ferrari V, Han Y, Aung N, Kenawy A, et al Recent trends and potential drivers of non-invasive cardiovascular imaging use in the United States of America and England. Front Cardiovasc Med2020;7:617771. https://doi.org/10.3389/fcvm.2020.617771
- 7. Timmis A, Townsend N, Gale CP, Torbica A, Lettino M, Petersen SE, et al European Society of Cardiology: cardiovascular disease statistics 2019. Eur Heart J2020;41:12–85. https://doi.org/10.1093/eurheartj/ehz859
- 8. Cosyns B, Garbi M, Separovic J, Pasquet A, Lancellotti PEducation Committee of the European Association of Cardiovascular Imaging Association (EACVI). Update of the echocardiography core syllabus of the European Association of Cardiovascular Imaging (EACVI). Eur Heart J Cardiovasc Imaging2013;14:837–9. https://doi.org/10.1093/ehjci/jet140
- 9. Petersen SE, Almeida AG, Alpendurada F, Boubertakh R, Bucciarelli-Ducci C, Cosyns B, et al Update of the European Association of Cardiovascular Imaging (EACVI) core syllabus for the European cardiovascular magnetic resonance certification exam. Eur Heart J Cardiovasc Imaging2014;15:728–9. https://doi.org/10.1093/ehjci/jeu076
- 10. Gimelli A, Neglia D, Schindler TH, Cosyns B, Lancellotti P, Kitsiou A. Nuclear cardiology core syllabus of the European Association of Cardiovascular Imaging (EACVI). Eur Heart J Cardiovasc Imaging2015;16:349–50. https://doi.org/10.1093/ehjci/jeu297
- 11. Nieman K, Achenbach S, Pugliese F, Cosyns B, Lancellotti P, Kitsiou A. Cardiac computed tomography core syllabus of the European Association of Cardiovascular Imaging (EACVI). Eur Heart J Cardiovasc Imaging2015;16:351–2. https://doi.org/10.1093/ehjci/jeu298
- 12. Fox K, Achenbach S, Bax J, Cosyns B, Delgado V, Dweck MR, et al Multimodality imaging in cardiology: a statement on behalf of the task force on multimodality imaging of the European Association of Cardiovascular Imaging. Eur Heart J2019;40:553–8. https://doi.org/10.1093/eurheartj/ehy669
- 13. Ooues G, Plummer C, Hall J, Lawson C, Price S, Smith R, et al How to succeed in the EEGC: a guide for trainees and their trainers. Heart2019;105:1044–5. https://doi.org/10.1136/heartjnl-2018-314496
- 14. Plummer C, Bowater S, Hall J, Lawson C, Ooues G, Price S, et al Behind the scenes of the European examination in general cardiology. Heart2019;105:889–90. https://doi.org/10.1136/heartjnl-2018-314495
- 15. Tanner FC, Brooks N, Fox KF, Gonçalves L, Kearney P, Michalis L, et al ESC core curriculum for the cardiologist. Eur Heart J2020;41:3605–92. https://doi.org/10.1093/eurheartj/ehaa641
- 16. Yong E, Manoharan K, Gent D. The European examination in core cardiology in focus: evaluation and recommendations using educational theory. J Eur CME2022;11:2055266. https://doi.org/10.1080/21614083.2022.2055266
- 17. Natale L, Vliegenthart R, Salgado R, Bremerich J, Budde RPJ, Dacher JN, et al Cardiac radiology in Europe: status and vision by the European Society of Cardiovascular Radiology (ESCR) and the European Society of Radiology (ESR). Eur Radiol2023;33:5489–97. https://doi.org/10.1007/s00330-023-09533-z