Introduction
Congenital auricular deformities are classified either as malformations or as deformations. Malformations are characterized by partial absence of the skin or cartilage, resulting in a constricted or underdeveloped pinna developing in the embryonic period. Auricle with deformities is fully developed, but misshapen pinnae caused by external forces. , The correction for malformation requires operative procedures to rebuild a new auricle, whereas deformed auricle can be treated not only with otoplasty but also with nonsurgical management, including ear molding, with fewer complications and higher success rates. , To date, the EarWell neonatal auricle deformity correction system is considered to be the widely used molding device and has shown superior results. - The EarWell ear molding system was first introduced to China in 2015. However, the cost for the EarWell device is around 10 000 RMB in China and cannot be covered by any medical insurance plan. Therefore, the wide application of EarWell ear molding was hindered by the exorbitant price. Recently, some domestic ear moldings for treatment of auricular deformities were developed in China and are much cheaper than the EarWell device. Here, we compared the therapeutic outcome of the LiangEar ear molding systems (made in China) and Earwell systems in the treatment of newborn auricular deformities. Moreover, the predictive factors were also investigated.
Patients and Methods
Patients
Between March 2017 and December 2017, 462 (522 ears) newborns, including 241 males and 221 females, were diagnosed with auricular deformities and received ear molding treatment at 2 tertiary hospitals in south China: Sun Yat-sen Memorial Hospital, Sun Yat-sen University, and Guangzhou Women and Children’s Medical Center. All infants were younger than the age of 6 months. Four types of ear deformities were included in the present study: cryptotia, prominent ear, helical rim abnormality, and cup ear. Infants with other systemic diseases were excluded. Baseline and posttreatment data were collected. The study was approved by the ethical review board of Sun Yat-sen Memorial Hospital and Guangzhou Women and Children’s Medical Center.
Ear Moldings
Two ear molding devices were used in the present study. One was the EarWell Infant Ear Correction System (Becon Medical Ltd, Naperville, Illinois), including auricle base, wide retractor, narrow retractor, conchal conformer, and posterior shell (Figure 1A), which was made of thermoplastic elastomer. The other was the LiangEar (Jiangsu Deviceland Medical Instrument Corp, Ltd, China), including ear cover, internal wall glue, cushion, ear base, lining glue, retractor, fixing pieces, external ear plug, and sponge (Figure 1B), which made of silica gel. Both devices were made in multiple sizes to fit different neonatal auricles. All infants were randomized into 2 groups to receive the selected device for treatment. Parents were fully informed, and permissions were obtained in advance.
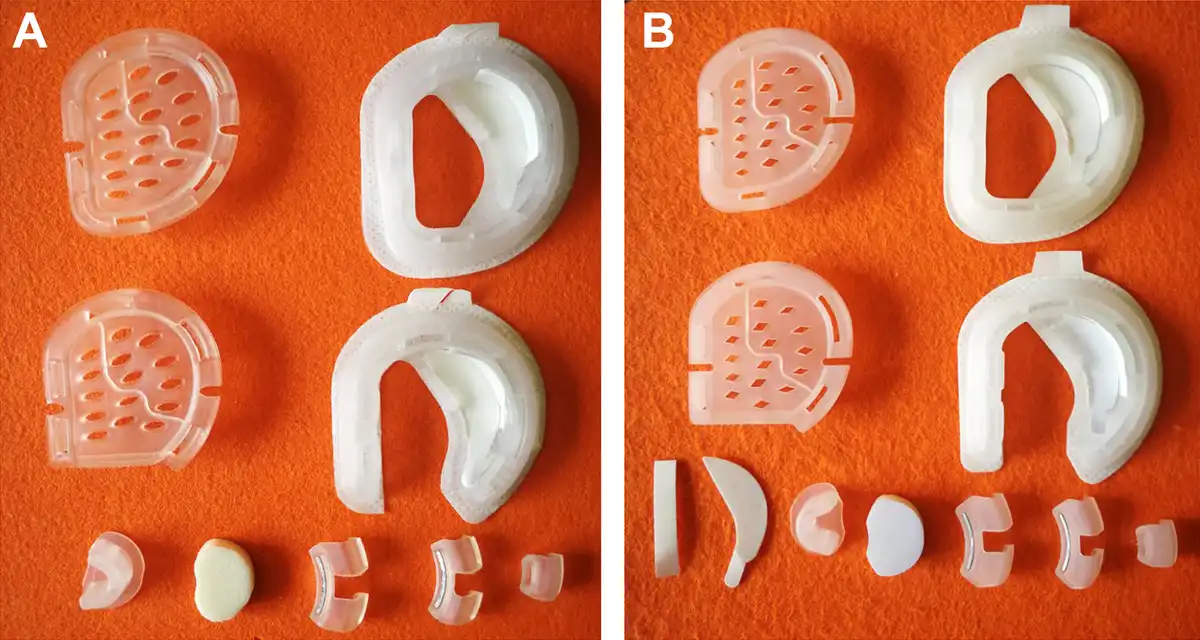
Figure 1
Two ear molding systems. A, The EarWell Infant Ear Correction System. B, The LiangEar Infant Ear Correction System.
Treatment and Evaluation
The 2 ear molding devices were installed by Dr Haidi Yang at Sun Yat-sen Memorial Hospital and Dr Xiaoya Wang at Guangzhou Women and Children’s Medical Center. All infants were scheduled for weekly follow-up to monitor auricle changes and to modulate the devices in order to obtain better correcting conditions. Infants wore the splinting for 24 hours per day. The splinting stopped only when serious skin problems such as erosion or eczema occurred. After management of skin lesions, the treating clinicians should replace the devices immediately and extend the duration of treatment depending on the correction progress. The splinting was performed continuously until 1 week after normalization of the auricle anatomy was achieved, and it was stopped after an 8-week treatment maximally even when no correction occurred. Six months after treatment, the cosmetic outcome was graded as good, fair, or poor by the treating clinicians (Table 1).
Statistical Analysis
The results were analyzed using SPSS 22.0 (Chicago, Illinois). Analysis of variance was used for comparisons between the groups. Logistic regression analysis was used to define prognosis factors. P values <.05 were considered statistically significant.
Results
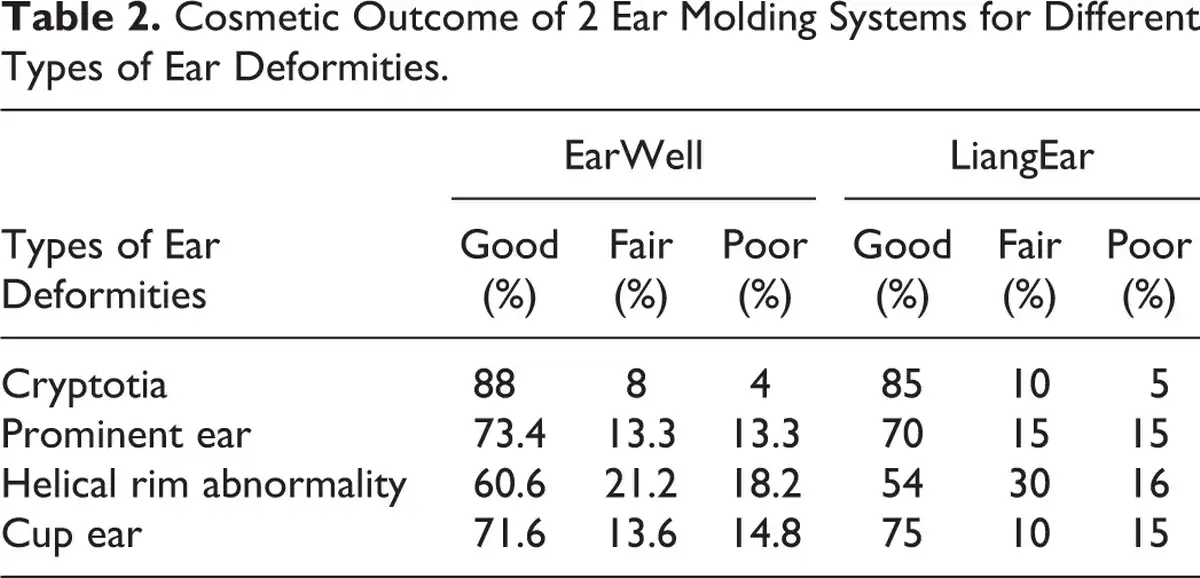
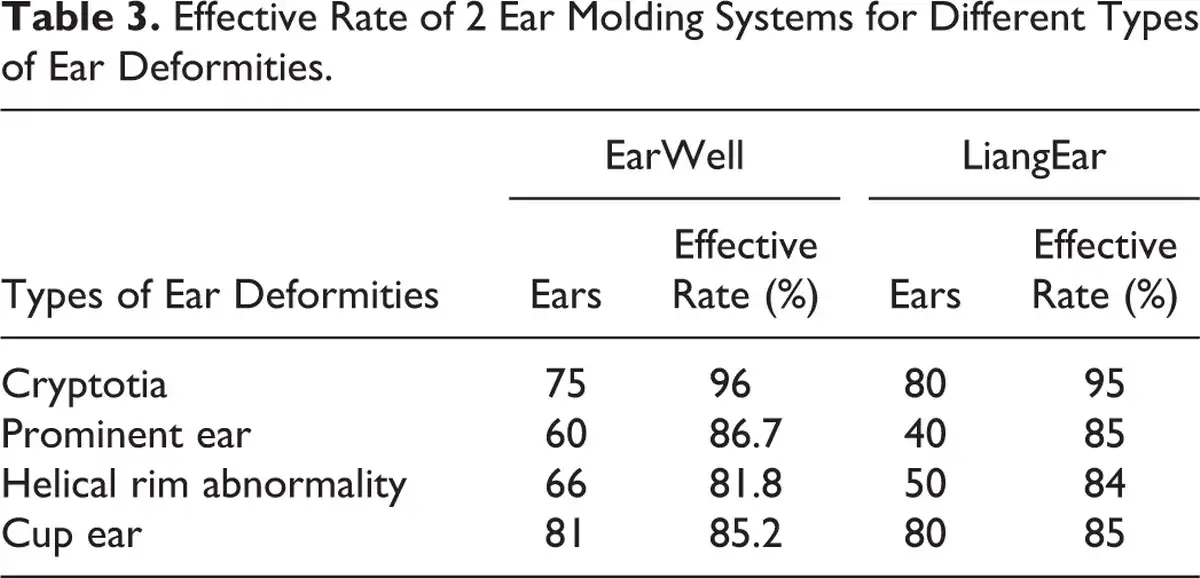
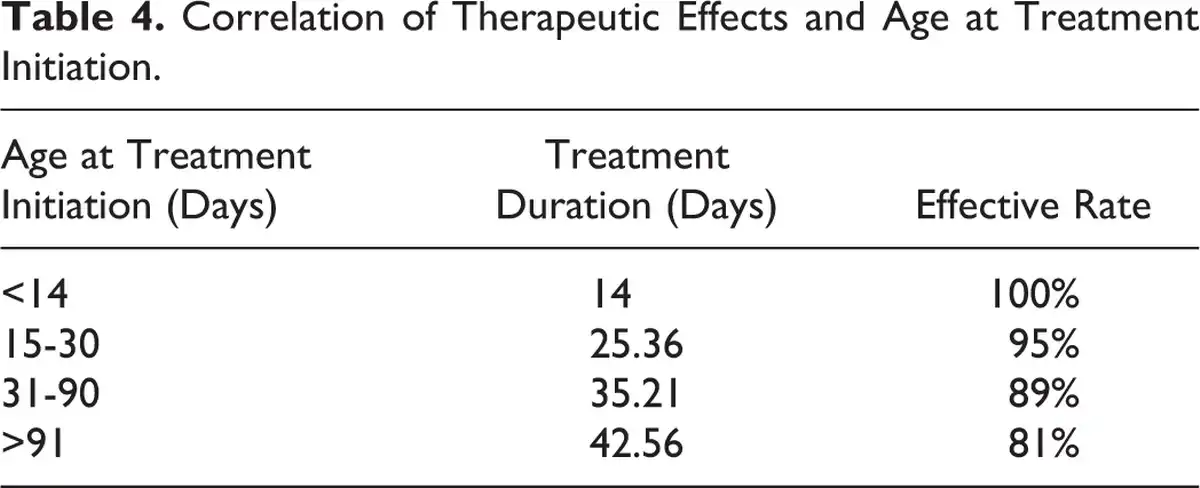
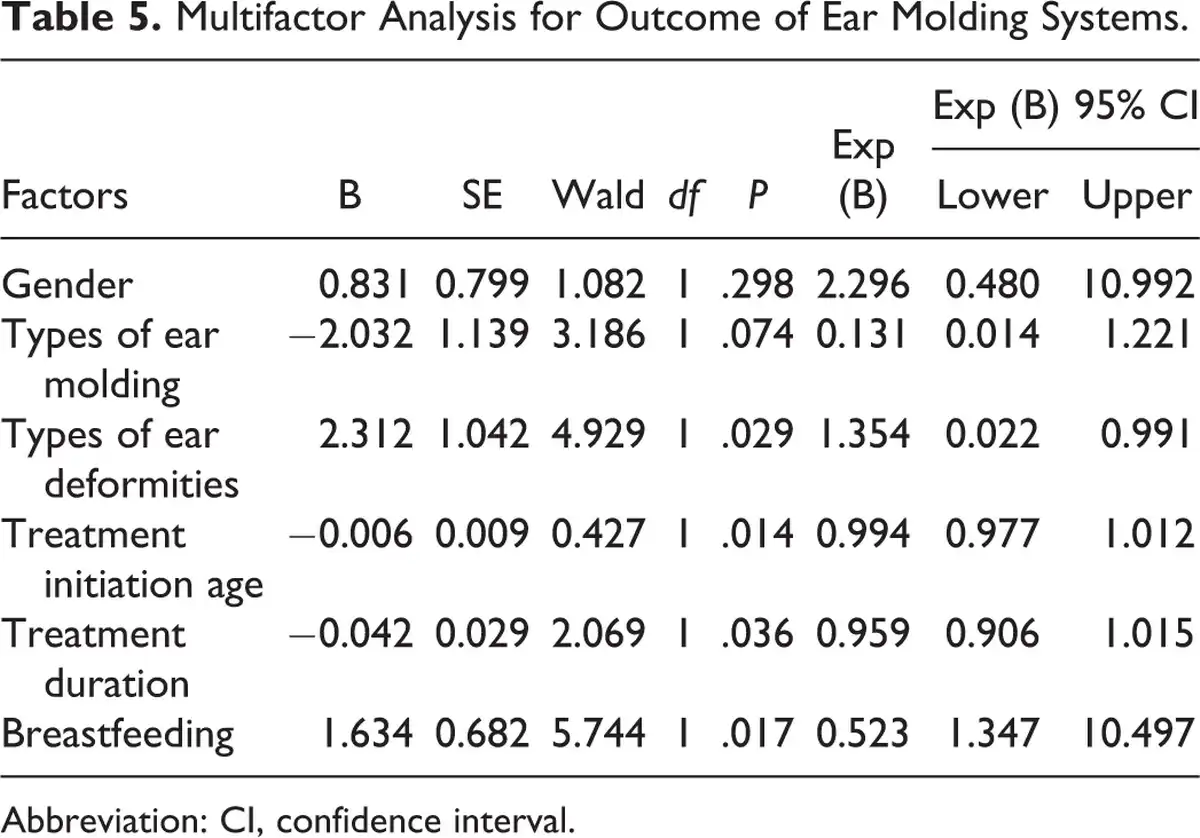
Two hundred eighty-two ear (250 infants) deformities were treated with the EarWell system, while 250 (212 infants) ear deformities were treated with the LiangEar system. The age for initiation of ear molding treatment ranged from 12 to 112 days. The posttreatment outcome of 2 ear molding systems for 4 types of ear deformities is shown in Table 2. The effective rate (outcome graded as good and fair) of the EarWell system was 96%, 86.7%, 81.8%, and 85.2% for cryptotia, prominent ear, helical rim abnormality, and cup ear, respectively. Similarly, the effective rate of the LiangEar system was 95%, 85%, 84%, and 85% for cryptotia, prominent ear, helical rim abnormality, and cup ear, respectively (Table 3). There is no difference in effective rate between 2 ear molding systems (P > .05). The typical treatment outcome of 2 ear molding systems is demonstrated in Figures 2 and 3. Notably, the costs for the LiangEar systems were half as much as those for the EarWell systems (5000 RMB vs 10 000 RMB). In addition, our findings showed that effective rate achieved 100% if treatment initiated when infants younger than 14 days of age (Table 4). The Multivariate regression analysis showed that earlier time points at treatment initiation, mild auricular deformities, longer treatment duration, and breastfeeding were the most significant predictive factors for a better outcome (P < .05). The type of ear molding and gender showed no influence in the treatment effects (P > .05; Table 5). Complications were found in 12 ears treated with the EarWell system and 11 ears treated with the LiangEar system, most of which were minor superficial excoriations and eczema. These skin lesions healed with the use of local antibiotics.

Figure 2
Typical results of the EarWell ear molding for different types of ear deformities. A and B, Before and after treatment for cryptotia. C and D, Before and after treatment for cup ear. E and F, Before and after treatment for helical rim abnormality. G and H, Before and after treatment for prominent ear.
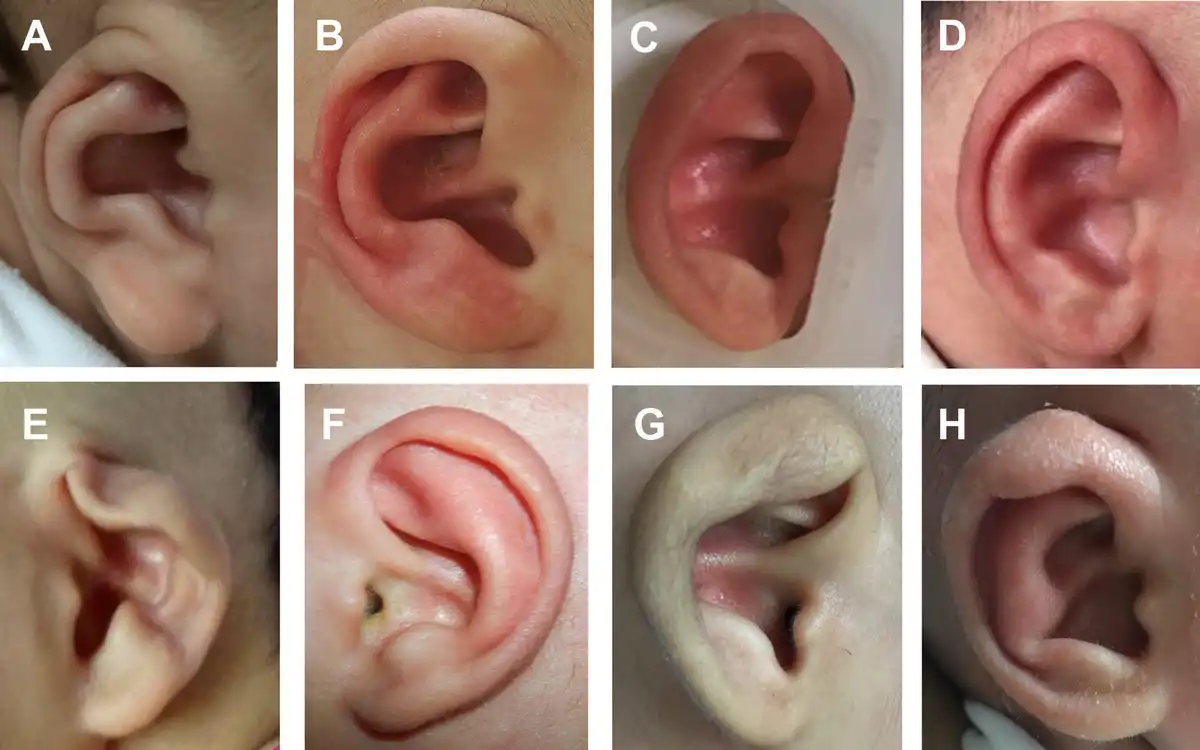
Figure 3
Typical results of the LiangEar ear molding for different types of ear deformities. A and B, Before and after treatment for cryptotia. C and D, Before and after treatment for prominent ear. E and F, Before and after treatment for helical rim abnormality. G and H, Before and after treatment for cup ear.
Discussion
The prevalence of auricular deformities is considered to be ∼11.5 per 10 000 births. It is estimated that more than 500 000 infants with auricular deformities needs to be treated in China every year. Traditionally, auricular deformities have been corrected surgically at ∼6 years of age. , Recently, nonsurgical management by ear molding has emerged as a favorable approach for newborn auricular deformities. -, The most widely used ear molding systems in the world are the EarWell Infant Ear Correction System. It is an approved adhesive device that attaches to the skin of child to mold the malformed ear into a normal anatomical shape. The EarWell system has shown much better outcomes in correction of auricular deformities than previous molding techniques or otoplasty. , The EarWell system has been introduced in China since 2015. However, the costs for the EarWell device are around 10 000 RMB in China, which is beyond the affordability of most parents from rural area in China. Therefore, many infants in rural China failed to take the advantage of this nonsurgical intervention to correct their auricular deformities. Fortunately, some domestic ear molding devices have been developed in China since recent 5 years, and the greatest strength of these products is much cheaper than the EarWell system and most parents in rural China can afford them. However, the efficacy of the domestic ear molding on auricular deformities has not been evaluated widely.
To the best of our knowledge, this is the first study to compare the effect of domestic and imported ear molding systems in China. Our findings indicated both ear molding systems showed substantial efficacy in the treatment of newborn auricular deformities. The effective rate was comparable between the EarWell and the LiangEar systems, while the costs for the LiangEar systems were much less than those for the EarWell systems. Multivariate regression analysis showed that earlier intervention and less severe auricular deformities results in a better outcome. To achieve satisfactory outcome, timing of ear molding is most important. The ideal intervention of auricular deformities is started within the first 2 weeks after birth. Circulating levels of maternal estrogen and tissue hyaluronic acid, which favor newborn ear malleability, peak during the first 72 hours after birth, and decline to baseline by 6 weeks of age, when the auricle becomes more elastic and firm. ,, Our results also demonstrated that effective rate was as high as 100% if the initiation is within the first 14 days after birth and dropped progressively when the intervention initiation delayed. Moreover, less severe auricular deformities results in better outcomes was found in our study, which is consisted with previous studies. , Our results indicated cryptotia auricle required shorter treatment duration than other types of deformities, with the highest effective rate of 96% among all types of deformity. Relatively, lower effective rate was achieved in prominent ear, cup ear, and helical rim abnormality, which are relatively more complex deformities. Interestingly, our results indicated breastfeeding is also significant predictive factors for a better outcome, this may due to the residual estrogen in the milk, which delays the decline in the circulating estrogen levels in the infants.
Minor complications, including local compressions, rashes, skin lesions, infections, and bleeding, are reported in 5% of the infants who treated with ear molding. In this study, infants had fewer complications during treatment. The most common complications were skin lesions and rashes, all of which were managed soon after the discontinuation of ear molding and specific treatment. Most complications of this splinting treatment occurred in infants older than 30 days.
In conclusion, the LiangEar and EarWell ear molding had remarkable and comparable therapeutic effects on neonatal auricular deformities. The LiangEar ear molding system is more suitable for infants with auricular deformities from rural China for lower costs. The type of auricle deformity and the age at starting correction were the main factors affecting the efficacy.
Declaration of Conflicting Interests The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Guangzhou Science and Technology Foundation (201903010088) and the National Natural Science Foundation of China (81970887).
Hao Xiong
https://orcid.org/0000-0003-3733-8083
Haidi Yang
https://orcid.org/0000-0002-7193-9598
References
- 1. Tan ST, Abramson DL, MacDonald DM, Mulliken JB. Molding therapy for infants with deformational auricular anomalies. Ann Plast Surg. 1997;38(3):263–268.
- 2. Byrd HS, Langevin CJ, Ghidoni LA. Ear molding in newborn infants with auricular deformities. Plast Reconstr Surg. 2010;126(4):1191–1200.
- 3. Porter CJ, Tan ST. Congenital auricular anomalies: topographic anatomy, embryology, classification, and treatment strategies. Plast Reconstr Surg. 2005;115(6):1701–1712.
- 4. Yotsuyanagi T, Yokoi K, Urushidate S, Sawada Y. Nonsurgical correction of congenital auricular deformities in children older than early neonates. Plast Reconstr Surg. 1998;101(4):907–914.
- 5. Matsuo K, Hayashi R, Kiyono M, Hirose T, Netsu Y. Nonsurgical correction of congenital auricular deformities. Clin Plast Surg. 1990;17(2):383–395.
- 6. Matsuo K, Hirose T, Tomono T, et al. Nonsurgical correction of congenital auricular deformities in the early neonate: a preliminary report. Plast Reconstr Surg. 1984;73(1):38–51.
- 7. Doft MA, Goodkind AB, Diamond S, DiPace JI, Kacker A, LaBruna AN. The newborn butterfly project: a shortened treatment protocol for ear molding. Plast Reconstr Surg. 2015;135(3):577e–583e.
- 8. Tapan M, Bulam H, Igde M, Singin S, Ünlü RE. A simple method of neonatal ear molding for treatment of Stahl ear deformity. J Craniofac Surg. 2015;26(8):e802–e803.
- 9. Anstadt EE, Johns DN, Kwok AC, Siddiqi F, Gociman B. Neonatal ear molding: timing and technique. Pediatrics. 2016;137(3):e20152831.
- 10. Schultz K, Guillen D, Maricevich RS. Newborn ear deformities: early recognition and novel nonoperative techniques. Semin Plast Surg. 2017;31(3):141–145.
- 11. Lennon C, Chinnadurai S. Nonsurgical management of congenital auricular anomalies. Facial Plast Surg Clin North Am. 2018;26(1):1–8.
- 12. Rozanski C, Rousso JJ. Congenital ear malformations: effectively correcting cryptotia with neonatal ear molding. Ear Nose Throat J. 2017;96(9):359–360.
- 13. Ullmann Y, Blazer S, Ramon Y, Blumenfeld I, Peled IJ. Early nonsurgical correction of congenital auricular deformities. Plast Reconstr Surg. 2002;109(3):907–913; discussion 14-15.
- 14. Mohammadi AA, Imani MT, Kardeh S, Karami MM, Kherad M. Non-surgical management of congenital auricular deformities. World J Plast Surg. 2016;5(2):139–147.
- 15. Leonardi A, Bianca C, Basile E, et al. Neonatal molding in deformational auricolar anomalies. Eur Rev Med Pharmacol Sci. 2012;16(11):1554–1558.
- 16. Chang CS, Bartlett SP. A simplified nonsurgical method for the correction of neonatal deformational auricular anomalies. Clin Pediatr (Phila). 2017;56(2):132–139.