
Figure
No caption available.
EVOLUTION OF THE UNDERSTANDING OF MYOPIA
Aristotle (384-322 bc) was the first one to describe short sightedness or myopia in his "The Generation of Animals", in which he mentions '‘Animals with prominent eyes do not see well from a distance, but those with small eyes placed in a hollow recess are able to see things at a distance because movement does not get scattered into space but follows a straight course. Thus, keen sight means :(a) the ability to see from a distance, and (b) distinguishing as accurately as possible the difference of objects which are seen, and these faculties do not occur together.[]
Galen (AD 130-200) then tried to explain myopia based on the theory of humours which was believed until about 1600s.[] Kepler, for the first time in 1604, gave an optical explanation of myopia along with the description of the optics of concave lenses. In 1611, Kepler suggested that occupation might also be a major factor influencing refraction, leading to the concept of school myopia.[]
Pathological description of degenerative myopia was only first described in 1801 by Antonio Scarpa. He was a prominent scholar who greatly contributed to the fields of otolaryngology, orthopedics, ophthalmology, neuroanatomy, and surgery.[] His ophthalmology textbook titled 'The Principal Diseases of the Eye' was one of the most popular books in the 19th century and included illustrations with plates engraved after his own drawings (Figure 1). Although he described the findings, but it is interesting to note that he was not aware that the eyes belong to myopic patients.
Figure 1
Antonio Scarpa (1752-1832) with the Cover page of Saggio di Osservazioni e d'Esperienze Sulle Principali Malattie Degli Occhi, 1801.
However, the pathological and ophthalmoscopic correlations of degenerative myopia happened only fifty years later by von Graefe in 1854.[]
ETIOLOGY OF DEGENERATIVE MYOPIA AND ITS LINKAGE TO POSTERIOR STAPHYLOMA
Ida Mann in 1957 hypothesized that there occurs an arrest in the development of sclera during the fifth month of fetal development. As a result of which the posterior sclera remains thin. Thin sclera along with the normal intraocular pressure leads to stretching of the posterior sclera causing aneurysmal dilatation and development of posterior staphyloma.[] Vogt in 1924 had proposed another theory suggesting degenerative myopia to be an overgrowth of the neurosensory retina, which however contrasts with the actual clinical scenario in these eyes.[] Gruenwald in 1944 determined retinal pigment epithelium to be the baseline factor central to the development of coloboma, a condition analogous to posterior staphyloma.[]
With this background, Blach et al in 1965 explained the linkage of degeneration of pigment epithelium or abnormal pigment epithelium and weak posterior sclera leading to staphyloma formation in eyes with degenerative or pathological myopia (Figure 2).[]
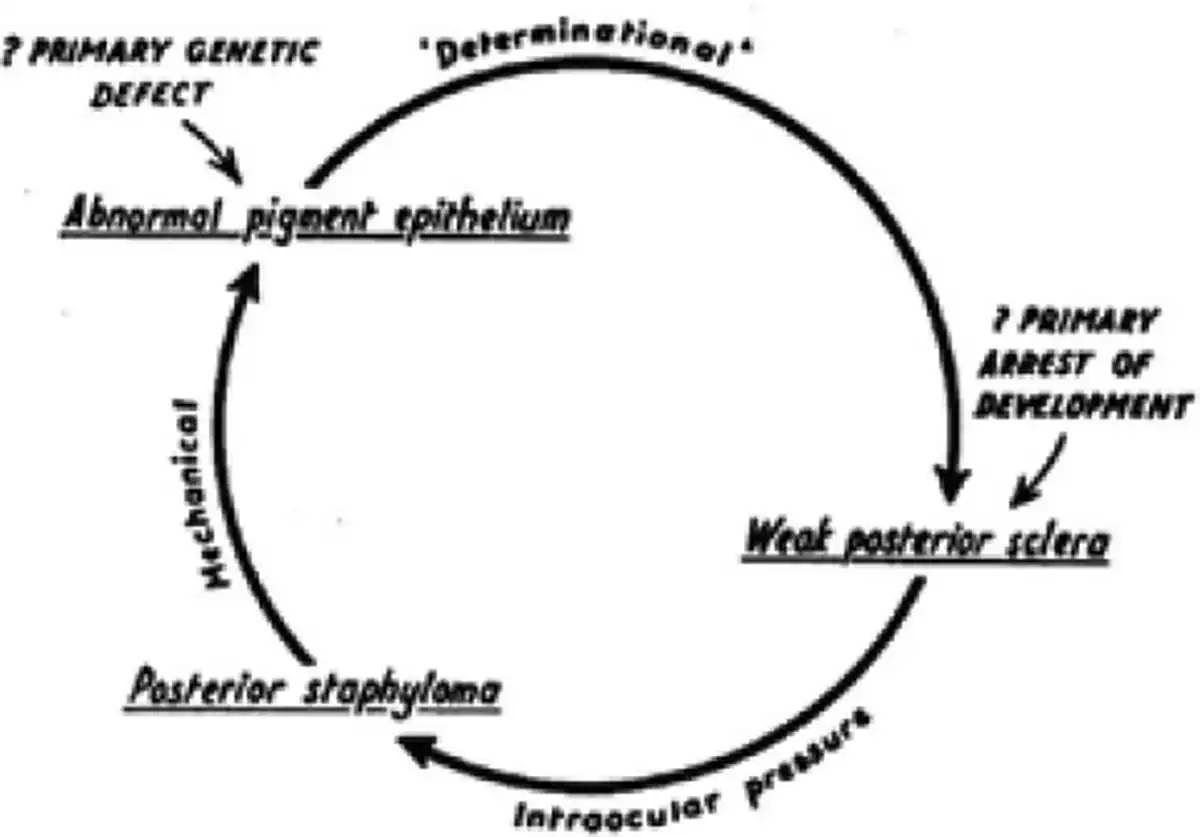
Figure 2
Illustration by Blach et al9 explaining the linkage of degeneration of pigment epithelium or abnormal pigment epithelium and weak posterior sclera leading to staphyloma formation in eyes with degenerative or pathological myopia.
POSTERIOR STAPHYLOMA AND ITS TYPES
Curtin and Karlin studied myopic eyes in detail and described five fundus changes which were associated with increased axial length are - Optic nerve crescent, chorioretinal atrophy, Fuchs's spots, Lacquer cracks and posterior staphyloma. The area of staphyloma has been described as a pale ectatic area of the fundus with prominent choroidal vasculature compared to the rest of the fundus. []
During their study, 1437 eyes were divided into 3 groups - Group I (less than or up to 19 years), Group II (20-39 years) and Group III (>40 years). They found greatest prevalence of posterior staphyloma in Group III with eyes more than 26.5 mm. They also observed a highly statistically significant regression coefficient for development of staphyloma in eyes measuring 26.5 to 36.6 mm (p<0.01).[]
Further, Curtin described various morphological types of posterior staphylomas, their prevalence, and their effect on the visual acuity of the affected eyes. Figure 3 describes a composite of different types of staphylomas as illustrated by Brian J. Curtin in 1977 - 5 types (type I through V) of primary and 5 types (type VI through X) of secondary staphylomas.[]

Figure 3
A composite figure of different types of staphylomas as illustrated by Brian J. Curtin in 1977 - 5 types (type I through V) of primary and 5 types (type VI through X) of secondary staphylomas
They concluded that the presence of posterior staphyloma forms the basis of pathological myopia and urges a careful and detailed stereoscopic evaluation of the posterior fundus in every myopic eye.
Financial disclosure
None
Conflict of Interest
None
Acknowledgements
Nil
REFERENCES
- 1. Aristotle (c. 384-332 BC) Generation of Animals. Trans. A L Peck. London. 1943; Book 5.
- 2. Galen C (c. AD 130-200) De usupartiumcorporishumani. In: Medicorum grccorum opera quae exstant. Ed.C G Kuhn. Leipzig. 1822;7:338.
- 3. Kepler J (1604)Ad vitellionem paralipomena. Frankfurt (1611) Dioptrice. Augsburg
- 4. Andrzej Grzybowski. Antonio Scarpa (1752-1832): Father of Italian ophthalmology. European Journal Of Ophthalmology. 2014.
- 5. Von Graefe A: Zwei Sektionsbefunde bei Sclerotico-choroiditis posterior und Bemer-kunger uber diese Kramkheit. Albrecht von Graefes Arch Ophthalmol. 1854; 1: 390–401.
- 6. Mann I. Developmental Abnormalities of the Eye. 2nd ed. London. 1957.
- 7. Vogt A. Ber. dtsch. Ophth. Ges. 1924;44:67.
- 8. Groenwald P. Amer. J. Anat. 1944;74:217.
- 9. Blach, et al. The concepts of Degenerative Myopia. Section of Ophthalmology. 58, 1965.
- 10. Curtin BJ, Karlin DB: Axial length measurements and fundus changes of the myopic eye. Part 1. Theposteriorfundus. TransAm OpthalmalSoc 68:312–334,1970.
- 11. Curtin B.J., 1977. The posterior staphyloma of pathologic myopia. Transactions of the American Ophthalmological Society 75, 67–86