Cannabis is one of the most widely used psychoactive substances. It has a rich history spanning thousands of years and varying representations throughout human civilization. Cannabis is mainly associated with three species of flowering plants belonging to the canabenaceae family, namely sativa, indica, and ruberalis. The plants are indigenous to Central Asia and the Indian subcontinent, where their earliest use dates back to at least the third century BC., The more prevalent term ‘marijuana’ typically refers to the dried leaves, stems, and flowering buds of the two more commonly consumed strains of sativa and indica. A few active components of cannabis, namely delta-9-tetrahydrocannabinol (THC), cannabinol (CBN), and cannabidiol (CBD), have been found to produce its intoxicating effects, which include feelings of euphoria, altered perception, relaxation, and wellbeing.–, In India, cannabis is commonly known to have three distinct derivatives; a) ganja (marijuana), the dried flower buds or fruits of the female cannabis plant, b) charas (hashish), the resinous exudation secreted by the plant, and c) bhang, a grinded paste of only the matured leaves.,
The use of cannabis has steadily grown in recent years, and more than 200 million people worldwide used cannabis in 2019 alone. It remains the most widely cultivated and trafficked illicit substance worldwide. In India, according to a nationwide survey, 31 million people (2.8% of the total population) reported using cannabis in 2018, and 0.25% (2.5 million) also showed signs of cannabis dependence. It is a significant increase compared to the estimates from a previous nationwide drug use survey in 2004, which reported cannabis use in 8.7 million Indians (3% of the total population). Like global patterns, cannabis remains the third most common substance of use in India alongside alcohol and tobacco, making it the most widely used illicit substance., There is also significant gender disparity in cannabis use in India, with 5% of males and only 0.6% of females reporting its use in the previous year.
Historical and Sociocultural Underpinnings of Cannabis use in India
The history of cannabis use is rooted in the Asian subcontinent. The indigenous strain of Cannabis indica has been growing freely along the Himalayan foothills and adjacent plains of India for centuries., The use of cannabis is a significant part of the religious lives of Hindus from mostly India and Nepal, and it has been represented in various Hindu scriptures. The earliest mention of Bhanga (cannabis preparation) is from the Atharva Veda (2000 BC to 1400 BC), where it is described as a sacred grass alongside alternate connotations of it as Indracana (Food of Gods), Vijaya (Victory), and Amrita (gift)., – In the Sushruta Samhita (600 AD), derivatives of cannabis were advocated as valuable medicines useful in treating certain phlegmatic ailments. Even to this day, the consumption of cannabis is regarded as auspicious during the annual Hindu festivals of Shivaratri, Krishna Ashtami, Kali puja, and Holi and is an essential part of certain religious observances., These historical and mythological accounts underscore the notions of cannabis as a valuable medicinal herb, a source of life force and euphoria, and a means for spiritual accord with the Gods., Interestingly, the current debates in the West regarding the medicinal value of cannabis had already preexisted in the Indian subcontinent.
The use of cannabis has been reported in India for at least a few thousand years; however, it was only in the 1800s that cannabis cultivation and use expanded rapidly in India and worldwide as nonpsychoactive hemp emerged as a valuable cash crop., The British rulers of India commissioned the mass cultivation of cannabis for hemp, which subsequently increased the rates of cannabis use as well., , Although the commercial use of hemp fiber grew obsolete as societies eventually shifted to steel, the recreational use of cannabis had spread to most parts of the world by then due to colonial conquests and trade., [See Warf (2014) for detailed historical geography of cannabis] The rise in cannabis use led to the formulation of the Indian Hemp Drugs Commission Report in 1894, and it is regarded as one of the first systematic studies on cannabis use. It concluded that only very heavy use of cannabis led to drastic physical, mental, and moral effects, not intermittent use., The following decades saw an unrestricted increase in cannabis cultivation and use, which peaked during the 1960s in India and Nepal. However, India passed the Narcotic Drugs and Psychotropic Substances Act in 1985, effectively banning the cultivation, production, and consumption of cannabis along with 70 other narcotic and psychotropic drugs., – This was after cannabis use became increasingly regulated and prohibited in the US and European countries, and India followed suit as a signatory to the UN Single Convention on Narcotic Drugs (1961).
Despite the legal prohibitions, cannabis remains the highest consumed and trafficked and frequently seized illicit substance in India., India is also known to have one of the lowest retail prices of cannabis globally., The Indian cities of Mumbai and Delhi are ranked amongst the top ten cities of the world in cannabis consumption., The consumption of cannabis derivatives, particularly bhang, has valuable religious and cultural connotations among Indians and thus remains widely accepted in Indian communities. In line with the global trend toward decriminalizing cannabis use, the support for legalizing cannabis in India for medical and recreational purposes has been gradually growing. Legislation for its medicinal and commercial use was also proposed in the Indian Parliament in 2016. Two Indian states of Uttarakhand and Madhya Pradesh permitted the cultivation of cannabis for medicinal and industrial purposes in 2019. There have been efforts toward medicalizing cannabis, and the Central Government recently commissioned a council under the Ministry of Ayurveda, Yoga, Naturopathy, Unani, Sidha, and Homeopathy (AYUSH) to conduct scientific research on the efficacy of cannabis for various medical conditions., – With increasing cannabis legalization and decriminalization worldwide, India has joined the movement but the research on multiple facets of cannabis use in India appears inadequate and with gaps in terms of providing key information for molding policies on cannabis use. A substantial body of research has emerged in the West on the nature of cannabis, its patterns of use, psychological and physiological correlates of cannabis use disorders, and various treatment methods and their outcomes.– However, these areas have been largely unexplored among the Indian population. Cannabis use has multiple representations at historical, socio cultural and political levels in India, but high quality and credible scientific research on cannabis use has been lacking.
Need for a Review of Research on Cannabis use in India
Apart from the rare government-commissioned epidemiological and household surveys, the level of scientific research on cannabis use in India has been very rudimentary at best, as evidenced by the scientific literature on cannabis use emerging from India. For a country that produced one of the first recorded accounts of the medicinal uses of cannabis, – as well as the first systematic studies on psychosis related to cannabis use, , the contribution from the Indian scientific community to recent cannabis literature is dismal. In India, cannabis use is firmly intertwined with people’s sociocultural lives. Future resolutions toward legalization or decriminalization of cannabis use need to be rooted in scientific evidence based on ground realities. At this critical juncture in India’s history of cannabis use, it remains imperative to evaluate the research efforts made so far to guide cannabis use policies and provide insights for future research.
In the following sections, original research studies on cannabis use from India have been reviewed. Electronic databases of PubMed, EBSCO host, ProQuest, and Google Scholar were searched for relevant articles using Boolean functions combining three key terms of ‘cannabis,’ ‘marijuana,’ and ‘India.’ Related keywords of ‘substance use,’ ‘drug use,’ ‘bhang,’ ‘ganja,’ and specific geographical locations from India were also used during the search. Specific inclusion criteria were set for selecting studies which were, a) original research studies using Indian participants, b) cannabis use and/or its dynamics as study variables, and c) date of publication between 1986 and 2020. 1985 was taken as the cut-off because the NDPS Act was passed in 1985, indicating a significant shift in socio-political contexts surrounding cannabis use, which this review has attempted to capture. Approximately 1500 research titles were scanned, out of which full texts of 100 articles were accessed and studied. The review was limited to quantitative original research studies and excluded published case studies and clinical case descriptions of cannabis-related conditions. The review also excluded many useful commentaries and review studies from India on cannabis-related psychosis and psychopathology, which had produced some key insights on cannabis use in India.– Based on the nature of the articles and the selection criteria, a total of 29 research studies were finalized for review. The selected research articles were reviewed and discussed under the following three themes; a) Prevalence of cannabis use, b) Psychological and psychiatric correlates of cannabis use, and c) Cannabis use in treatment settings.
Prevalence of Cannabis use in India
Most of the Indian research studies found on cannabis use were prevalence studies, where the prevalence of cannabis use had been assessed alongside a range of different substances or health behaviors. In most Indian studies identified, the research designs were rudimentary; samples were small and as per convenience, and statistical analyses were limited to only descriptive ones. In Table 1, the studies that reported only the prevalence of cannabis use among community samples have been described and evaluated.
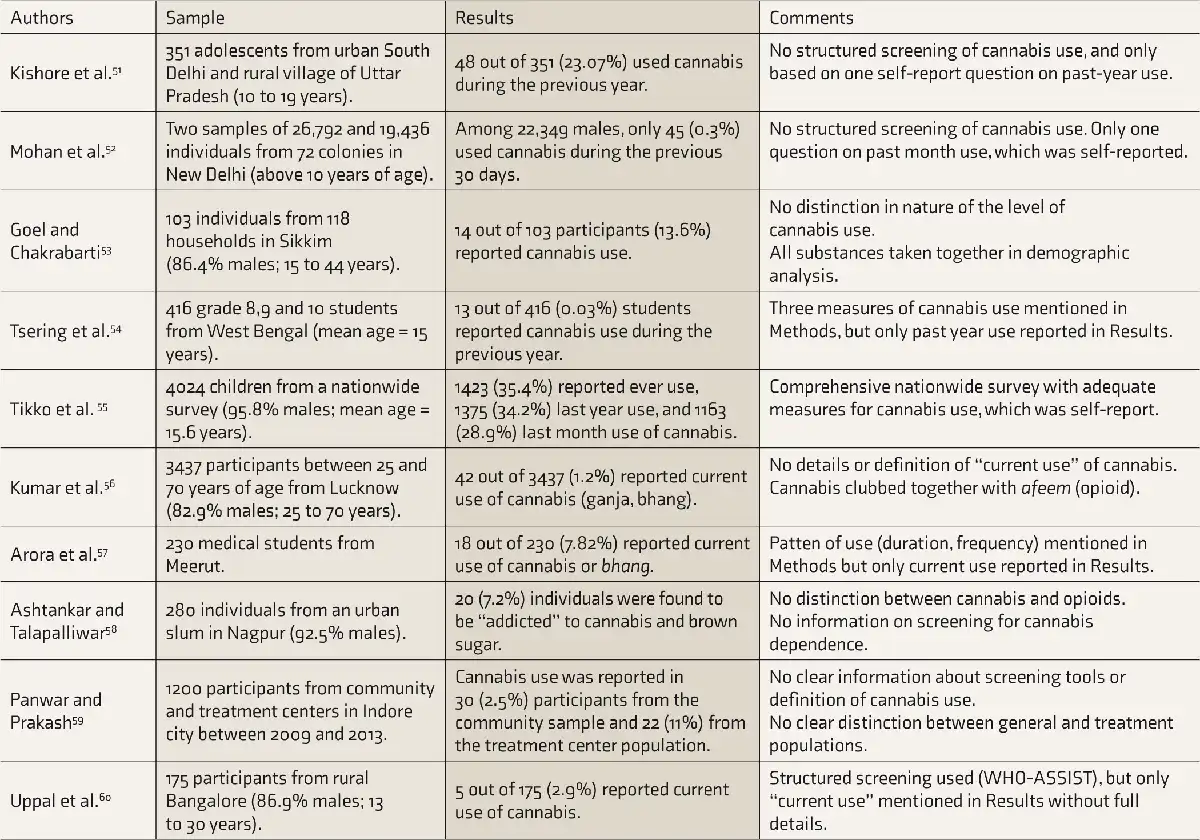
WHO, World Health Organization; ASSIST, alcohol, smoking and substance involvement screening test
The primary objective of most studies reviewed in Table 1 had been to estimate rates of substance use, of which cannabis was only a minor part. In most instances, the assessment of cannabis use was limited to basic measures of lifetime use, previous year use, or previous month use; however, a few studies did not clarify even that., , Most studies did not include descriptions of the nature of administration, frequency and intensity of use, or period of use. Only two studies distinguished between cannabis types (bhang, ganja) in their measures., Two studies had even combined cannabis use along with opioid use in a single category., Apart from two studies, none used standard screening instruments and mostly relied on self-report interviews., Six out of the ten prevalence studies had total sample sizes below 500, and males made up all or significant proportions of the samples in all ten studies. Four studies reported on prevalence among adolescents, and the rates of cannabis use were similar to adults., , , The pooled prevalence of cannabis use ranged 0.3-28.9% for the previous month and 2.5-34.2% for the previous year. Dube and Dhingra (2020) estimated the prevalence rate of cannabis use to be 6.7%, based on a pooled estimate from five Indian studies. Given these disparities in estimates of cannabis use across research studies, it becomes difficult to ascertain the true prevalence. Thus, the state-commissioned national surveys have proved to be more reliable and representative.,
Psychological and Psychiatric Correlates of Cannabis use
Throughout the modern history of cannabis, the role of cannabis use as a predictor or consequence of psychosis has been extensively studied. In fact, the first reports of the ‘cannabis psychosis’ phenomenon emerged from India and even preceded the Indian Hemp Drugs Commission Report of 1894. At first, the observations were specific to India, and the condition was communicated as the ‘Indian hemp insanity’ by Ewens in 1904. The study by Chopra et al. (1942) on the association between cannabis and mental diseases was one of the first scientific inquiries on cannabis psychosis. There were many research studies on psychiatric and psychological correlates of cannabis use prior to the NDPS Act (1985).– However, no convincing evidence for the links between cannabis use and psychosis was reported, and only heavy or chronic use was associated with psychotic symptoms. In the last three decades, research on cannabis use from the disciplines of psychology and psychiatry has produced consistent evidence for various psychological correlates of cannabis use and dependence, as well as the effects of cannabis on mental and physical health. In Table 2, eight original research studies that explored the psychological correlates of cannabis use among Indian samples have been listed.
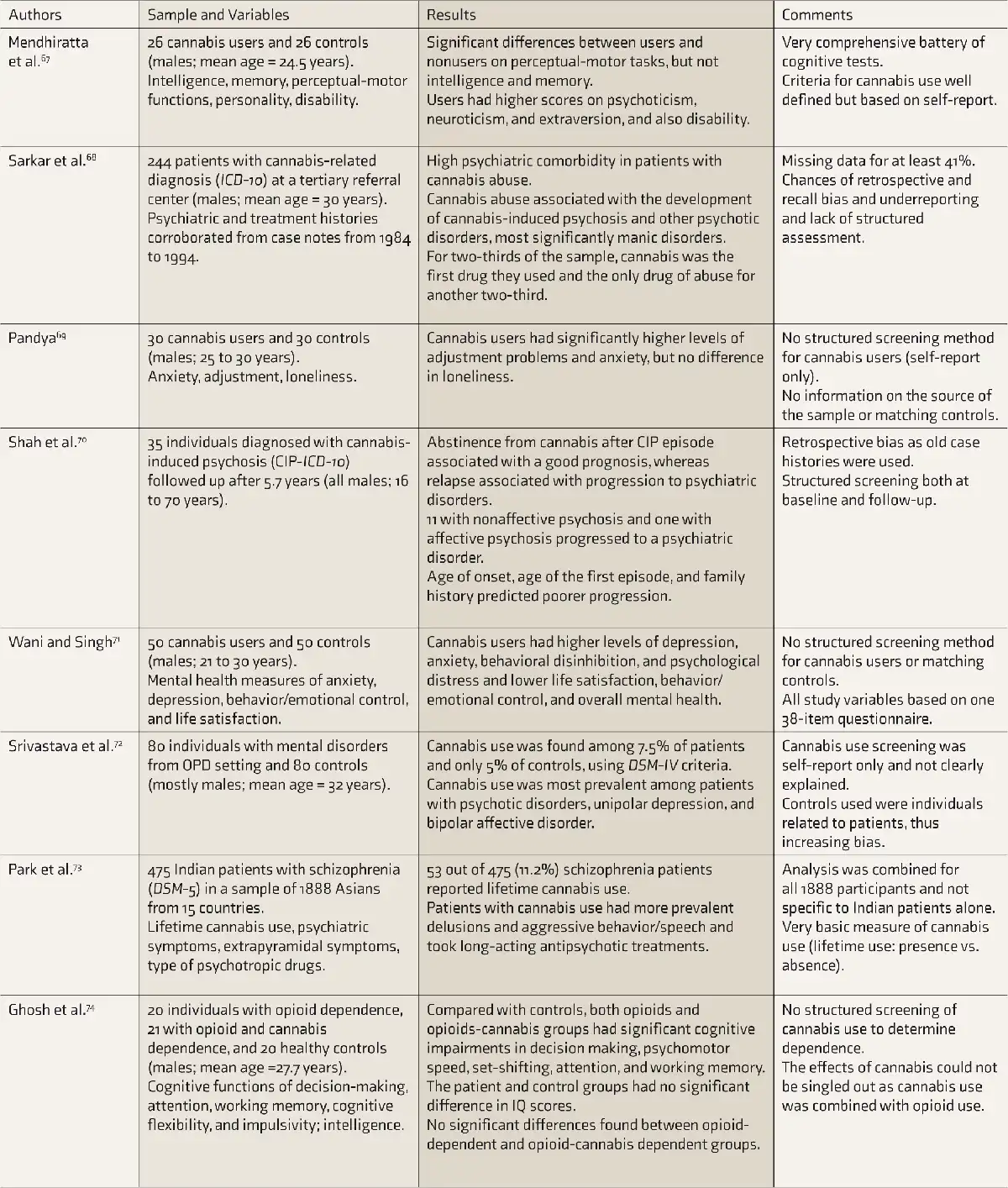
ICD, International Classification of Diseases; OPD, outpatient department; DSM, Diagnostic and Statistical Manual of Mental Disorders
In Table 2, six studies assessed cannabis use along with psychosis and other psychological conditions, and some degree of association was found.– Significant comorbidity was reported between cannabis use and psychiatric disorders, particularly psychosis-related conditions., , , Sarkar et al. (2003) comprehensively explored psychiatric comorbidity of cannabis use and found evidence for psychiatric conditions being significant precedents and consequences of cannabis use. Mixed results have been reported by studies from other countries as well. Singh and Balhara (2017), in their review of cannabis use and psychosis, found that Indian studies mostly described only acute episodes of psychosis characterized by positive and affective symptoms resulting from cannabis use. Two studies in this review also found evidence for cannabis use related to affective symptom conditions, particularly manic psychosis., Two studies examined cognitive functions and found significant differences in perceptual-motor functioning, but not intelligence, between users and healthy controls., In terms of methodological weaknesses, two studies utilized existing case notes and were prone to limitations of secondary data and recall biases., Use of basic cannabis-use screening measures was found in four studies., –, Apart from two studies, the remaining six had very small sample sizes as well.
Treatment of cannabis use
Cannabis use disorder has been recognized by the Diagnostic and Statistical Manual of Mental Disorders (DSM–5) as a legitimate mental health condition characterized by physiological adaptation, impaired behavioral control, and social and occupational impairment., Despite the growing notion of cannabis being safer than alcohol and tobacco, a sizable proportion of cannabis users become dependent on it and exhibit negative physical and psychological effects that require treatment., Numerous studies in recent years have reported on various treatment methodologies for cannabis use disorders, and cannabis derivatives have also been found to be useful in the treatment of other substance use disorders and in alleviating certain medical conditions., However, the scientific literature on cannabis use is still limited, particularly studies on interventions and treatment of cannabis-related conditions. The literature from India on cannabis use treatment is even sparse. There is a pressing need to determine effective strategies to prevent, delay, reduce, and treat cannabis abuse and dependence., In India, cannabis users also make up a significant proportion of individuals seeking treatment from deaddiction and rehabilitation centers every year., In Table 3, research studies exploring cannabis-use-related variables within substance use treatment programs in India have been reviewed.
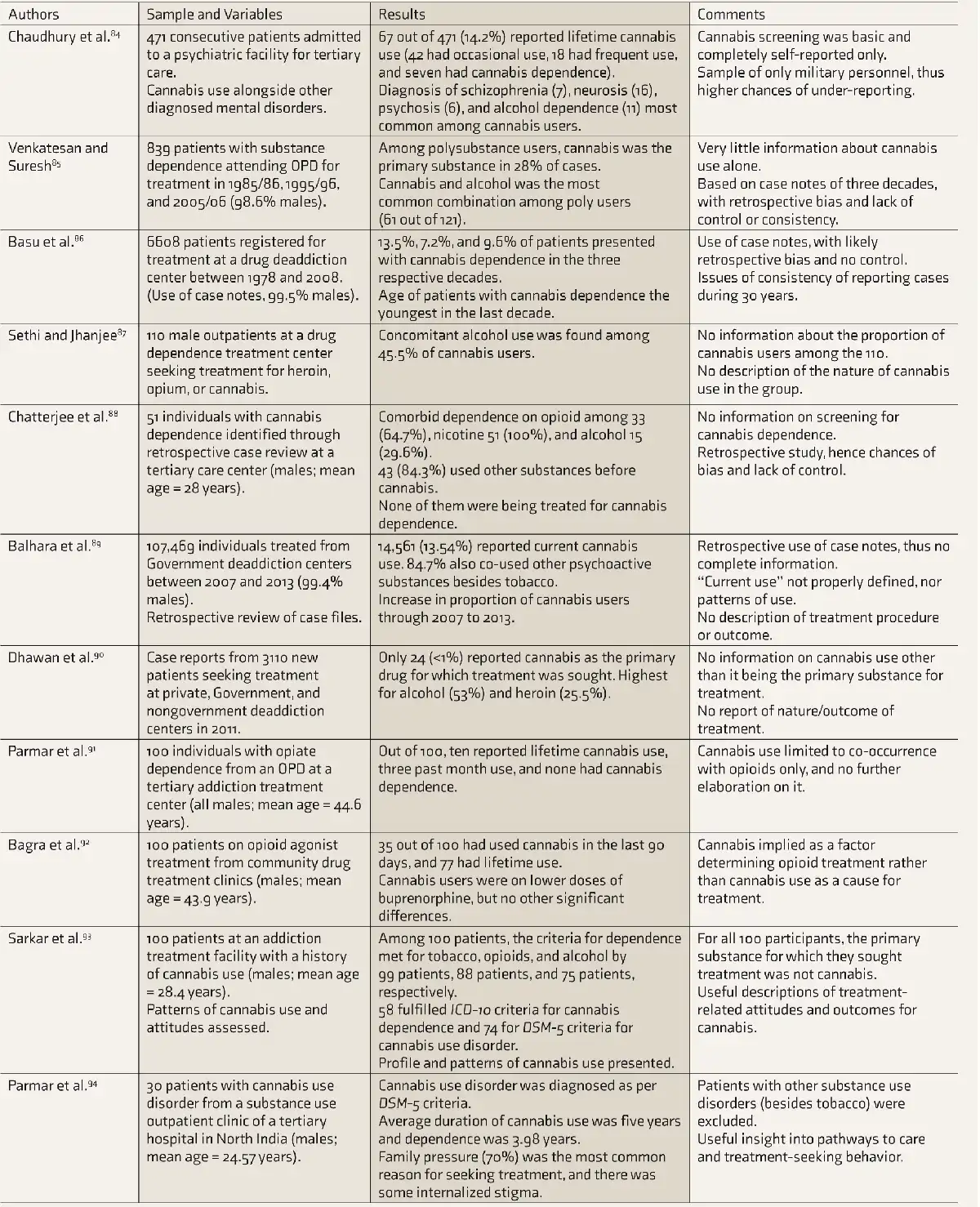
ICD, International Classification of Diseases; OPD, outpatient department; DSM, Diagnostic and Statistical Manual of Mental Disorders
From the studies reviewed in Table 3, it is apparent that cannabis abuse and dependence were not the primary reasons for approaching substance use treatment centers. It was mostly problems associated with alcohol or opioid use, and patients were found to have used cannabis or diagnosed with cannabis use disorder only during treatment., – Up to 13% of patients across the studies indicated cannabis as the primary substance for seeking treatment., , The studies revealed a high degree of polysubstance use, with high concurrent use and dependence on tobacco, alcohol, or opioids., –,– None of the studies addressed cannabis use or dependence in terms of treatment variables, and most of them only provided sociodemographic profiles of substance use patients in treatment. No research study from India was found that reported on the outcomes of psychosocial or psychiatric treatments for cannabis-use-related conditions.
Discussion
The present review highlights several salient aspects of the status of cannabis use research in India for the period between 1985 and 2021. Apart from studies on the association between cannabis use and psychosis, the overall research output on all aspects of cannabis use has been sparse and brief. Cannabis use often appears only as a subpart of substance use prevalence studies in India, along with sociodemographic associations of substance use. However, many of these studies lack scientific rigor due to the use of elementary designs and measures, small samples, and predominantly descriptive statistical analyses. The most comprehensive and representative prevalence estimates still come from government-commissioned national surveys conducted a couple of times every decade. There were a few Indian studies on psychiatric correlates of cannabis use but hardly any published literature on treatment methods and outcomes for cannabis dependence and related disorders. There remains huge scope for examining questions about cannabis use in India, and research conducted so far provides the best indication of limitations that need to be improved on.
The reviewed prevalence studies and the reports from national surveys reveal the extent of use of cannabis in India, with millions of active users at any given time. Among the illicit substances in India, the use of cannabis is significantly higher than opioids, inhalants, and prescription drugs. Given its unique sociocultural and political position in Indian society, the future course for cannabis use liberalization should be carefully outlined. Any stride towards legalization must consider the consequences of cannabis use rates exploding in the future, particularly among Indian youths. The proponents of cannabis usually point out that cannabis is less risky than alcohol and tobacco, which, although legal, still causes a great deal of personal and social harm., However, the health costs associated with tobacco and alcohol are largely attributed to their magnitude of use. Even with cannabis, there are a proportion of users who face negative physical and psychological consequences, which will only become more apparent with widespread use., The US, which has largely shaped the modern history of cannabis, is also one of the forerunners in cannabis medicalization and legalization for recreational use. The rate of its use there has already surpassed that of tobacco. Going forward, India must set its own cannabis narrative, incorporating its rich cultural and religious heritage surrounding cannabis use.
In recent years, Western countries have seen a proliferation of the use of cannabis derivative products and synthetic cannabis. Modern technologies have enabled scientists and cannabis cultivators to isolate and process different components of cannabis, particularly delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD), which have specific psychoactive properties and physical effects as well as different medicinal and recreational values. In places where cannabis is legalized for medicinal or recreational purposes, the use of CBD-based products such as oils and supplements has drastically increased in recent years. Decriminalization of cannabis use for medical and recreational purposes has led to better regulation of relative concentrations of the active components of various cannabis strains and derivative products, with scope for use across realms of wellness, recreation, pain or stress relief, and health. In India, the indigenous distinction between marijuana, bhang, and hashish has existed for centuries, and the three derivatives have considerable differences in concentrations of THC, CBD, and other components. However, none of the 29 reviewed studies made any significant distinction between the different modes of cannabis administration, the concentration of active components, or their relative effects. The medicalization of cannabis use in India began very recently, and almost all research studies reviewed in this article examined cannabis use as a negative health behavior or condition. With more Indian states permitting the cultivation of cannabis and hemp for medicinal purposes, several Indian startups have also begun selling cannabis-based products aimed at wellness and relief.–, Many have attempted to consolidate Western scientific evidence on concentrations of CBD and THC with practices and customs from the Hindu tradition, such as Ayurveda, to create uniquely Indian cannabis products.
One interesting fact that emerged from the review of the Indian research studies was the profound gender differences in cannabis use and the other substances. Large nationwide surveys have validated this. The rates of use of alcohol, tobacco, cannabis, and other illicit drugs are many times higher among Indian males than females., Among the 29 reviewed studies, all or most of the participants were male. A few reasons can be attributed for this phenomenon, the main one being the nature of social arrangements and gender roles in Indian communities, which are still rife with patriarchy. Women are still disadvantaged and underrepresented in education, occupation, policy-making, etc. The same has extended to substance use, with less access and negative perceptions and disapproval of women using substances. Males predominantly make up the substance use treatment population as well, and there are disproportionately fewer female-centered treatment and rehabilitation programs for cannabis use. This inevitably affects treatment-seeking and outcomes as well for women. However, the rate of substance use among Indian women has been increasing recently, particularly among younger women in the urban centers of the country. The difference in substance access, perceptions, and attitudes between the genders itself remains a worthwhile area for further research to elucidate the extent and reasons for the huge gender disparity.
Another important detail that emerged from the review was the lack of scientific and standardized assessment for cannabis use in research studies. In most of the articles reviewed, the inquiry for cannabis use status was limited to ordinal-level questions of lifetime use or a previous year or month of use. The nature of the use of cannabis remains a multifaceted variable with details of administration routes and dosage, intensity and frequency, subjective experiences, and progression to dependence characterizing further specifics. Many of those details are parts of standardized assessment tools such as the Alcohol, Smoking, and Substance Involvement Screening (ASSIST) by WHO and structured interview schedules based on the DSM 5 or ICD 10., , While it makes sense to include brief measures of cannabis use while estimating the prevalence of a range of different substances and allowing for large community-level assessments, there is also a dire need for systematic research studies to characterize cannabis use alone among large samples of Indians. Until now, research on cannabis has always been overshadowed by tobacco and alcohol. This warrants particular attention to cannabis use in future research to characterize its various dimensions and correlates properly.
There has been a surge in scientific research on various aspects of cannabis use in recent decades, pioneered by researchers in the US and Europe. Mainstream research has moved beyond simply estimating prevalence of cannabis use. Researchers are increasingly studying various aspects of cannabis use, such as the characterization of cannabis use profiles and cannabis use disorders,– association with other substances and polysubstance use,, and risk factors and predictors of use at various individual, family, and social levels.– Younger age groups have been the focus of cannabis use research, , and longitudinal studies have explored trajectories of cannabis use right from young age to adulthoo, when the consequences of long-term use become most apparent., The field of cannabis use research is burgeoning globally and the contribution from the Indian scenario is imperative. The social, cultural and political factors surrounding cannabis use in India are one of the most unique in the world. High-quality systematic research on these facets can help shed light on the intricacies of cannabis use that are still unexplored.
In terms of limitations of the review study, one major concern was the nature of the reviewed articles. Although three primary databases had been utilized (PubMed, EBSCO host, and ProQuest), which represent legitimate indexing bodies, there was a dearth of relevant studies, which led to the deployment of Google Scholar too. Since Google Scholar is not a standardized indexing body and is based primarily on crowd-sourced and web crawler data, research articles found through the same are of questionable quality. Nonetheless, an objective judgment was used to screen for low-quality publications. There is also the possibility that existing and relevant research studies were missed or not found through the conventional search strategies. Thus, the review is in no way exhaustive of all existing research studies fitting the inclusion criteria.
Recommendations and Future Directions
Based on the present review and considering the global context and current issues on cannabis use, the following recommendations for future research emerged. First, the extent of cannabis use in India needs to be monitored more rigorously through timely nationwide surveys involving large representative samples of various age, gender, region, and ethnic groups. The two most prominent recent national surveys assessed cannabis use alongside a range of psychoactive substances with the primary aim of determining only the prevalence of cannabis use across the country., There is a need for further nationwide surveys focusing on cannabis use, with consideration for administration routes, patterns of use, association with other substances, biopsychosocial correlates, and cultural/religious influences specific to India. The assessment and screening of cannabis use and related disorders also need to be standardized across treatment settings in India to ensure better monitoring. Health institutions remain the primary point of contact with cannabis users. There is huge scope to develop frameworks to record relevant details related to cannabis use and foster further research. This can aid in formulating effective treatment regimens and extending intervention efforts at the community level.
In terms of research on cannabis use in India, there is a need to determine the influence of indigenous practices on rates of cannabis use and also the various ways in which cannabis is represented in beliefs, rituals, and lifestyle among Indians. Cannabis has deep religious and sociocultural significance in India, and this ultimately influences people’s perceptions and use of cannabis despite it being illegal in India. More innovative research on different facets of cannabis use is needed, and central and state agencies must ensure the provision of necessary mechanisms to support and foster research on cannabis use. This includes easing administrative/legal hurdles, protection of participants, and direct funding for cannabis-use research. The policies on cannabis cultivation, distribution, and use must be aligned at the state and central levels to ensure standard implementation and jurisdiction.
Cannabis decriminalization in most modern societies started with medicalization, before recreational use was later permitted. This distinction needs to be carefully considered, along with the psychosocial effects of both, before any step towards full legalization of cannabis is made in India. With the emergence of cannabis-based products for a range of medical and health conditions in India, more scientific research is needed to test the effectiveness of cannabis and its related products as medicinal drugs and also gauge the extent of its negative effects. The rise in the use of CBD-based products and synthetic cannabis needs to be regulated until their short- and long-term effects on health can be determined through more scientific evidence grounded in high-quality indigenous research. Younger age groups and individuals with vulnerabilities to mental health disorders have the highest risks to negative consequences of cannabis use., , After decriminalizing cannabis in Western countries, there has been a dramatic rise in cannabis use among younger age groups. For any step towards propagating the medicinal or positive health effects of cannabis use in India, the increased health and social costs emerging from a higher prevalence of use should be carefully monitored. With rising cannabis use in India, more effective policies and regulations are also needed to prevent youths from initiating cannabis use. Subsequently, more scientific research is needed to determine the effects of cannabis use during adolescence and emerging adulthood.
Conclusion
Cannabis has a chequered history in India, one that has spanned thousands of years, and is associated with multiple connotations as medicine, divine herb, cash crop, and a drug of recreation or abuse. Only in the most recent parts of its Indian history was cannabis banned, its use and prevalence grew exponentially, and now it is on the verge of being legalized again. For a substance known to have an addiction propensity and distinct negative effects, there is still a lot we do not know about cannabis, and scientific research on it has picked up only in the recent decades. For a country with such unique history surrounding cannabis, the state of scientific research on cannabis in India is quite basic, as evident by the above review. There is a dire need for systematic and high-quality research on cannabis use, particularly to explore the influences of the sociocultural representations of cannabis on the rapidly growing rates of cannabis use initiation among Indians. Alcohol and tobacco are already huge social menaces in India, costing millions of lives and billions in the economy every year. It remains a collective responsibility of researchers, policy makers, economists, and citizens alike to prevent the same happening with cannabis.
Declaration of Conflicting Interests The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding The author received no financial support for the research, authorship, and/or publication of this article.
References
- 1. Behere AP, Behere PB, Rao TS. Cannabis: Does it have a medicinal value? Indian Journal of Psychiatry, 2017 ;59(3):262–63. https://dx.doi.org/10.4103%2Fpsychiatry.IndianJPsychiatry_208_17
- 2. Gokhale C, Bhardwaj R. Brief study of Cannabis sativa: A Review. International Journal of Information and Computing Science, 2018;5(8):123–30. http://www.ijics.com/gallery/a8.pdf
- 3. Hillig KW, Mahlberg PG. A chemotaxonomic analysis of cannabinoid variation in Cannabis (Cannabaceae). American Journal of Botany, 2004 ;91(6):966–75. 10.3732/ajb.91.6.966
- 4. Murray RM, Morrison PD, Henquet C, Di Forti M. Cannabis, the mind and society: the hash realities. Nature Reviews Neuroscience, 2007 ;8(11):885–95. 10.1038/nrn2253.
- 5. Sagar KA, Gruber SA. Marijuana matters: reviewing the impact of marijuana on cognition, brain structure and function, & exploring policy implications and barriers to research. International Review of Psychiatry, 2018 ;30(3):251–67. https://dx.doi.org/10.1080%2F09540261.2018.1460334
- 6. Tandon T. Drug Policy in India: Key developments since the UNGASS 2016. International Drug Policy Consortium. 2019 http://fileserver.idpc.net/library/India-drug-policy_FINAL.pdf
- 7. Osborne GB, Fogel C. Understanding the motivations for recreational marijuana use among adult Canadians. Substance Use & Misuse, 2008 ;43(3-4):539–572. 10.1080/10826080701884911
- 8. Chopra IC, Chopra RN. The Use of the Cannabis Drugs in India. United Nations Office on Drugs and Crime. 1957;4–29. https://www.unodc.org/unodc/en/data-and-analysis/bulletin/bulletin_1957-01-01_1_page003.html
- 9. United Nations Office on Drugs and Crime. World Drug Report 2021: Executive Summary. United Nations Publications 2021. http://www.unodc.org/unodc/en/data-and-analysis/wdr2021.html
- 10. Turner AR, Agrawal S. Marijuana Toxicity. In StatPearls (Internet), StatPearls Publishing, Treasure Island (FL), US. 2020. https://www.ncbi.nlm.nih.gov/books/NBK430823/
- 11. Ambekar A, Agrawal A, Rao R, Mishra AK, Khandelwal SK, Chadda RK, on behalf of the group of investigators for the National Survey on Extent and Pattern of Substance Use in India (2019). Magnitude of Substance Use in India. New Delhi: Ministry of Social Justice and Empowerment, Government of India.
- 12. Ray R. The Extent, Pattern and Trends of Drug Abuse in India. National Survey. Report submitted to Ministry of Social Justice and Empowerment, Government of India and United Nations Office on Drugs and Crime, Regional Office for South Asia. 2004. https://www.unodc.org/pdf/india/presentations/india_national_survey_2004.pdf
- 13. Gautham MS, Gururaj G, Varghese M, Benegal V, Rao GN, Kokane A, Chavan BS, Dalal PK, Ram D, Pathak K, Lenin Singh, RK. The National Mental Health Survey of India (2016): Prevalence, sociodemographic correlates and treatment gap of mental morbidity. International Journal of Social Psychiatry, 2020 ;66(4):361–372. 10.1177%2F0020764020907941
- 14. Murthy P, Manjunatha N, Subodh BN, Chand PK, Benegal V. Substance use and addiction research in India. Indian Journal of Psychiatry, 2010 ;52(Suppl1):S189. https://dx.doi.org/10.4103%2F0019-5545.69232
- 15. Mold A. Cannabis; Getting High: Marijuana Through the Ages. Cultural and Social History, 2018;15(1):152–4. 10.1080/14780038.2017.1415040
- 16. Touw M. The religious and medicinal uses of Cannabis in China, India and Tibet. Journal of Psychoactive Drugs, 1981 ;13(1):23–34. 10.1080/02791072.1981.10471447
- 17. Russo E. Cannabis for migraine treatment: the once and future prescription? An historical and scientific review. Pain, 1998 ;76(1-2):3–8. 10.1016/S0304-3959(98)00033-5
- 18. Aldrich MR. Tantric cannabis use in India. Journal of Psychedelic Drugs, 1977 ;9(3):227–33. 10.1080/02791072.1977.10472053
- 19. Godlaski TM. Shiva, lord of bhang. Substance Use & Misuse, 2012 ;47(10):1067–72. 10.3109/10826084.2012.684308
- 20. Charles M, Bewley-Taylor D, Neidpath A. Drug policy in India: Compounding harm. Briefing paper, The Beckley Foundation Drug Policy Programme (BFDPP) 2005;1–6. http://fileserver.idpc.net/library/BFDPP_BP_10_DrugPolicyIndia_EN.pdf
- 21. Dasgupta S. Legalization of Marijuana in India. Available at SSRN 2261316 2013 . https://dx.doi.org/10.2139/ssrn.2261316.
- 22. Biswas P, Mishra P, Bose D, Durgbanshi A. Cannabis: a neurological remedy or a drug of abuse in India. CNS & Neurological Disorders-Drug Targets (Formerly Current Drug Targets-CNS & Neurological Disorders), 2017 ;16(5):576–84. 10.2174/1871527316666170424115008.
- 23. Mikuriya TH. Marijuana in medicine: past, present and future. California Medicine, 1969 ;110(1):34. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1503422/
- 24. Warf B. High points: an historical geography of cannabis. Geographical Review, 2014;104(4):414–38. 10.1111/j.1931-0846.2014.12038.x
- 25. Mills JH. Cannabis Britannica: Empire, trade, and prohibition 1800-1928. Oxford University Press, Oxford, UK 2003.
- 26. Pisanti S, Bifulco M. Modern history of medical cannabis: from widespread use to prohibitionism and back. Trends in Pharmacological Sciences, 2017 ;38(3):195–8. 10.1016/j.tips.2016.12.002
- 27. Ayonrinde OA. Cannabis and psychosis: revisiting a nineteenth century study of ‘Indian Hemp and Insanity ‘in Colonial British India. Psychological Medicine, 2020 ;50(7):1164–72. 10.1017/S0033291719001077.
- 28. Mikuriya TH. Physical, mental, and moral effects of marijuana: the Indian Hemp Drugs Commission Report. International Journal of the Addictions, 1968 ;3(2):253–70. 10.3109/10826086809067437
- 29. Acharya SL, Howard J, Panta SB, Mahatma SS, Copeland J. Cannabis, Lord Shiva and Holy Men: Cannabis Use Among Sadhus in Nepal. Journal of Psychiatrists’ Association of Nepal, 2014;3(2):9–14. https://www.nepjol.info/index.php/JPAN/article/view/12379
- 30. Balhara YP, Mathur S. Bhang-beyond the purview of the narcotic drugs and psychotropic substances act. Lung India: Official Organ of Indian Chest Society, 2014 ;31(4):431. https://dx.doi.org/10.4103%2F0970-2113.142109
- 31. Bhalla A, Basu D, Singh S. Recreational drugs in India. Journal of Mahatma Gandhi Institute of Medical Sciences, 2015 ;20(1):20–30. 10.4103/0971-9903.151724
- 32. Chauhan AS. Criminalisation Of Marijuana Is A Remnant Of Older Times And An Orthodox Mind. Youth ki Awaaz, YKA Media Pvt Ltd 2020 . https://www.youthkiawaaz.com/2020/02/the-complicated-relationship-of-india-and-cannabis/
- 33. Das P. Drug Trafficking in India: A Case for Border Security. Institute for Defence Studies and Analyses, New Delhi 2012 . http://fileserver.idpc.net/library/OP_DrugTraffickinginIndia%20(1).pdf
- 34. United Nations. Report of the International Narcotics Control Board for 2018. United Nations: International Narcotics Control Board. 2019 . https://www.incb.org/documents/Publications/AnnualReports/AR2018/Annual_Report/Annual_Report_2018_E_.pdf
- 35. Kapil S. India is one of the major hubs for illicit drug trade. Down To Earth, 2019 . https://www.downtoearth.org.in/news/health/-india-is-one-of-the-major-hubs-for-illicit-drug-trade--63470
- 36. Cannabis and opium based drugs cheapest in India. The Times of India, 2017 . https://timesofindia.indiatimes.com/india/indian-drugs-cheapest-in-the-world/articleshow/59230170.cms
- 37. Sharma N. Delhi consumes more weed than Los Angeles, Mumbai more than London. Quartz India, 2019 . https://qz.com/india/1705970/delhi-mumbai-among-worlds-biggest-consumers-of-weed/
- 38. Tandon S. Delhi and Mumbai are among the world’s most stoned cities. Quartz India, 2018 . https://qz.com/india/1193934/delhi-and-mumbai-are-among-the-worlds-most-stoned-cities/
- 39. Bill for legalised supply of opium, marijuana cleared for Parliament. Hindustan Times, 2016 . https://www.hindustantimes.com/punjab/aap-mp-gandhi-s-bill-seeking-opium-legalisation-cleared-for-tabling-in-parliament/story-itanKX3vRrhuXJPdgnJD6N.html
- 40. Madhya Pradesh govt to legalise cannabis cultivation. Deccan Herald, 2019 . https://www.deccanherald.com/national/north-and-central/madhya-pradesh-govt-to-legalise-cannabis-cultivation-778282.html
- 41. Mehrotra PK. Is India losing out on a ready-to-boom cannabis market by not legalising its use? The Economic Times, India Times, 2018 . https://economictimes.indiatimes.com/industry/cons-products/tobacco/is-india-losing-out-on-a-ready-to-boom-cannabis-market-by-not-legalising-its-use/articleshow/66101561.cms?from=mdr
- 42. Singh K. Modi’s love for Ayurveda may be just the push marijuana needed in India. Quartz India, 2018 . https://qz.com/india/1474267/modis-ayurveda-push-may-promote-marijuana-use-in-india/
- 43. Temple EC, Brown RF, Hine DW. The ‘grass ceiling’: limitations in the literature hinder our understanding of cannabis use and its consequences. Addiction, 2011 ;106(2):238 10.1111/j.1360-0443.2010.03139.x
- 44. Sohn E. Safety-Balancing Acts. Nature. 2019;572(7771):S16–8. https://media.nature.com/original/magazine-assets/d41586-019-02530-7/d41586-019-02530-7.pdf
- 45. Chopra RN, Chopra GS, Chopra IC. Cannatis sativa in Relation to Mental Diseases and Crime in India. Indian Journal of Medical Research, 1942;30(1).
- 46. World Health Organization. The health and social effects of nonmedical cannabis use. WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland. 2016. https://www.who.int/substance_abuse/publications/msb_cannabis_report.pdf
- 47. Basu D, Malhotra A, Varma VK. Cannabis related psychiatric syndromes: A selective review. Indian Journal of Psychiatry, 1994 ;36(3):121. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2972478/pdf/IJPsy-36-121.pdf
- 48. Ghosh A, Basu D. Cannabis and psychopathology: The meandering journey of the last decade. Indian Journal of Psychiatry, 2015 ;57(2):140–149. 10.4103/0019-5545.158134
- 49. Parakh P, Basu D. Cannabis and psychosis: Have we found the missing links?. Asian Journal of Psychiatry, 2013 ;6(4):281–7. 10.1016/j.ajp.2013.03.012
- 50. Shrivastava A, Johnston M, Terpstra K, Bureau Y. Pathways to psychosis in cannabis abuse. Clinical Schizophrenia & Related Psychoses, 2015 ;9(1):30–5. 10.3371/csrp.shjo.030813
- 51. Kishore J, Singh A, Grewal I, Singh SR, Roy K. Risk behaviour in an urban and a rural male adolescent population. National Medical Journal of India, 1999 ;12:107–110. http://archive.nmji.in/archives/Volume-12/issue-3/original-articles-3.pdf
- 52. Mohan D, Chopra A, Sethi H. A rapid assessment study on prevalence of substance abuse disorders in metropolis Delhi. Indian Journal of Medical Research, 2001 ;114:107–114. https://pubmed.ncbi.nlm.nih.gov/11873400/
- 53. Goel A, Chakrabarti A. Prevalence and sociodemographic correlates of substance use in a rural community in Sikkim, North East India: Results from a pilot population survey. Journal of Substance Use, 2010 ;15(1):13–23. 10.3109/14659890902964005
- 54. Tsering D, Pal R, Dasgupta A. Licit and illicit substance use by adolescent students in eastern India: Prevalence and associated risk factors. Journal of Neurosciences in Rural Practice, 2010 ;1(02):076–81. https://dx.doi.org//10.4103/0976-3147.71721
- 55. Tikko VK, Dhawan A, Pattanayak RD, Chopra A. Assessment of Pattern and Profile of Substance Use among Children in India. National Commission for Protection of Child Rights (NCPCR). 2014. https://movendi.ngo/wpcontent/uploads/2019/05/68106596.pdf
- 56. Kumar S, Mehrotra D, Mishra S, Goel MM, Kumar S, Mathur P, Choudhary K, Pandey CM. Epidemiology of substance abuse in the population of Lucknow. Journal of Oral Biology and Craniofacial Research, 2015 ;5(3):128–33. https://dx.doi.org/10.1016%2Fj.jobcr.2015.08.010
- 57. Arora A, Kannan S, Gowri S, Choudhary S, Sudarasanan S, Khosla PP. Substance abuse amongst the medical graduate students in a developing country. The Indian Journal of Medical Research, 2016 ;143(1):101. https://dx.doi.org/10.4103%2F0971-5916.178617
- 58. Ashtankar HJ, Talapalliwar MR. Felt need and treatment-seeking barriers among substance abusers in urban slum area in Central India. Indian Journal of Psychological Medicine, 2017 ;39(4):436–40. https://dx.doi.org/10.4103%2F0253-7176.211760
- 59. Panwar Y, Prakash MM. Narcotic drug abuse patterns of Indore city with special reference of opium, marijuana and cannabis. International Journal of Pharmacology and Biological Sciences, 2017;11(1):23–8. https://search.proquest.com/docview/1937767519?accountid=38885
- 60. Uppal G, Peethala P, Gopalakrishnan G. Prevalence of substance abuse among adolescents and young adults in rural Bangalore- an epidemiological study. Journal of Evidence Based Medicine and Healthcare, 2018;5(51):3510–3. https://dx.doi.org/10.18410/jebmh/2018/716
- 61. Dube S, Dhingra N. An Overview: Prevalence of Cannabis Abuse in India. International Journal of Contemporary Medical Research, 2020;7(2):B1–4. http://dx.doi.org/10.21276/ijcmr.2020.7.2.3
- 62. Thara R, Padmavati R, Srinivasan TN. Focus on psychiatry in India. The British Journal of Psychiatry, 2004 ;184(4):366–73. https://pdfs.semanticscholar.org/606b/c898555e2028bc3291766ef2c37d447f4d9b.pdf
- 63. Goel DS, Captain S, Netto TB. Cannabis: The habit and psychosis. Indian Journal of Psychiatry, 1975 ;17(4):238–43.
- 64. Sethi BB, Trivedi JK, Singh H. Long term effects of cannabis. Indian Journal of Psychiatry, 1981;23(3):224–9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3012947/pdf/IJPsy-23-224.pdf
- 65. Grossman W. Adverse reactions associated with Cannabis products in India. Annals of internal medicine, 1969;70(3):529–33. 10.7326/0003-4819-70-3-529
- 66. Radhakrishnan R, Wilkinson ST, D’Souza DC. Gone to pot–a review of the association between cannabis and psychosis. Frontiers in Psychiatry, 2014 ;5:54. 10.3389/fpsyt.2014.00054
- 67. Mendhiratta SS, Varma VK, Dang R, Malhotra AK, Das K, Nehra R. Cannabis and Cognitive Functions: a re-evaluation study. British Journal of Addiction, 1988 ;83(7):749–53. 10.1111/j.1360-0443.1988.tb00506.x
- 68. Sarkar J, Murthy P, Singh SP. Psychiatric morbidity of cannabis abuse. Indian Journal of Psychiatry, 2003 ;45(3):182–8. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2952166/pdf/IJPsy-45-182.pdf
- 69. Pandya I. Adjustment, anxiety and loneliness in cannabis users and controls. Indian Journal of Health & Wellbeing, 2017 ;8(8). https://search.proquest.com/docview/1961766780?accountid=38885
- 70. Shah D, Chand P, Bandawar M, Benegal V, Murthy P. Cannabis induced psychosis and subsequent psychiatric disorders. Asian Journal of Psychiatry, 2017 ;30:180–184. 10.1016/j.ajp.2017.10.003
- 71. Wani IA, Singh B. Mental health and cannabis abusers of Kashmir Valley. Journal of Psychology and Psychotherapy, 2017;7(2):1–5. 10.4172/2161-0487.1000297
- 72. Srivastava M, Jain S, Patel A. Substance use among outdoor treatment-seeking patients with mental illness: A case–control study from a tertiary care hospital of northern India. Journal of Education and Health Promotion. 2018;7(75). 10.4103/jehp.jehp_97_17
- 73. Park SC, Oh HS, Tripathi A, Kallivayalil RA, Avasthi A, Grover S, Tanra AJ, Kanba S, Kato TA, Inada T, Chee KY. Cannabis use correlates with aggressive behavior and long-acting injectable antipsychotic treatment in Asian patients with schizophrenia. Nordic Journal of Psychiatry, 2019 ;73(6):323–30. 10.1080/08039488.2019.1632381
- 74. Ghosh A, Basu D, Mattoo SK, Kumar Rana D, Roub F. Does Cannabis Dependence Add on to the Neurocognitive Impairment Among Patients With Opioid Dependence? A Cross-Sectional Comparative Study. The American Journal on Addictions, 2020 Mar;29(2):120–8. 10.1111/ajad.12986
- 75. Singh S, Balhara YP. A review of Indian research on co-occurring cannabis use disorders & psychiatric disorders. The Indian Journal of Medical Research, 2017 ;146(2):186. https://dx.doi.org/10.4103%2Fijmr.IJMR_791_15
- 76. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing 2013 https://dsm.psychiatryonline.org/doi/book/10.1176/appi.books.9780890425596
- 77. Patel J, Marwaha R. Cannabis Use Disorder, In StatPearls (Internet), StatPearls Publishing, Treasure Island (FL), US. 2019 . https://www.ncbi.nlm.nih.gov/books/NBK538131/
- 78. Palamar JJ, Fenstermaker M, Kamboukos D, Ompad DC, Cleland CM, Weitzman M. Adverse psychosocial outcomes associated with drug use among US high school seniors: a comparison of alcohol and marijuana. The American Journal of Drug and Alcohol Abuse, 2014 ;40(6):438–46. 10.3109/00952990.2014.943371
- 79. Salloum NC, Krauss MJ, Agrawal A, Bierut LJ, Grucza RA. A reciprocal effects analysis of cannabis use and perceptions of risk. Addiction, 2018 ;113(6):1077–85. 10.1111/add.14174
- 80. Lau N, Sales P, Averill S, Murphy F, Sato SO, Murphy S. A safer alternative: Cannabis substitution as harm reduction. Drug and Alcohol Review, 2015 ;34(6):654–9. 10.1111/dar.12275
- 81. Bottorff JL, Bissell LJ, Balneaves LG, Oliffe JL, Kang HB, Capler NR, Buxton JA, O’Brien RK. Health effects of using cannabis for therapeutic purposes: a gender analysis of users’ perspectives. Substance Use & Misuse, 2011 ;46(6):769–80. 10.3109/10826084.2010.537732
- 82. Mahu IT, Doucet C, O’Leary-Barrett M, Conrod PJ. Can cannabis use be prevented by targeting personality risk in schools? Twenty-four-month outcome of the adventure trial on cannabis use: a cluster-randomized controlled trial. Addiction, 2015 ;110(10):1625–33. 10.1111/add.12991
- 83. Mittal S, Ch’ien JMN. Developing Community Drug Rehabilitation. Rapid Assessment Study of Drug Abuse in Target Communities in India. Report submitted to Ministry of Social Justice and Empowerment, Government of India, International Labour Organisation and United Nations International Drug Control Programme, Regional Office for South Asia. 1998.
- 84. Chaudhury S, Sudarsanan S, Salujha SK, Srivastava K. Cannabis use in psychiatric patients. Medical Journal Armed Forces India, 2005;61(2):117–20. https://dx.doi.org/10.1016%2FS0377-1237(05)80004-8
- 85. Venkatesan J, Suresh SS. Substance dependence: Decades apart in a teaching hospital. Indian Journal of Psychiatry, 2008 ;50(2):100–5. https://dx.doi.org/10.4103%2F0019-5545.42396
- 86. Basu D, Aggarwal M, Das PP, Mattoo SK, Kulhara P, Varma VK. Changing pattern of substance abuse in patients attending a de-addiction centre in north India (1978-2008). The Indian Journal of Medical Research, 2012 ;135(6):830. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3410210/
- 87. Sethi H, Jhanjee S. Use of alcohol among treatment seeking illicit drug users in India. Journal of Mental Health and Human Behaviour 2014 ;19(1):29–31. https://dx.doi.org//10.4103/0971-8990.143887
- 88. Chatterjee B, Quraishi R, Jain R. Sociodemographic and Drug Use Characteristics of Treatment-seeking Cannabis Users at a Tertiary Care Center in India. Addictive Disorders & Their Treatment, 2014 ;13(3):110–5. https://dx.doi.org//10.1097/ADT.0b013e31828bf7f2
- 89. Balhara YP, Mishra A, Sethi H, Singh S, Khandelwal SK. Time trends of cannabis use among treatment-seeking individuals at government de-addiction centers across India over a period of 7 years. Indian Journal of Psychological Medicine, 2016 ;38(4):331–5. https://dx.doi.org/10.4103%2F0253-7176.185961.
- 90. Dhawan A, Chopra A, Ray R. Preferences for treatment setting by substance users in India. Indian Journal of Psychological Medicine, 2016 ;38(1):42–5. https://dx.doi.org/10.4103%2F0253-7176.175105
- 91. Parmar A, Patil V, Sarkar S, Rao R. An observational study of treatment seeking users of natural opiates from India. Substance Use & Misuse, 2018 ;53(7):1139–45. 10.1080/10826084.2017.1400564
- 92. Bagra I, Krishnan V, Rao R, Agrawal A. Does cannabis use influence opioid outcomes and quality of life among buprenorphine maintained patients? A cross-sectional, comparative study. Journal of Addiction Medicine, 2018 ;12(4):315–20. 10.1097/adm.0000000000000406
- 93. Sarkar S, Parmar A, Singh A. An exploratory study of cannabis use pattern and treatment seeking in patients attending an addiction treatment facility. Indian Journal of Psychiatry, 2020 ;62(2):145. https://dx.doi.org/10.4103%2Fpsychiatry.IndianJPsychiatry_132_19
- 94. Parmar A, Gupta P, Bhad R. An exploratory study of clinical profile, stigma and pathways to care among primary cannabis use disorder patients in India. Journal of Substance Use, 202;27(1):74–9. 10.1080/14659891.2021.1897695
- 95. Johnston LD, Miech RA, O’Malley PM, Bachman JG, Schulenberg JE, Patrick ME. Monitoring the Future national survey results on drug use, 1975-2018: Overview, key findings on adolescent drug use. Institute for Social Research. 2019. https://eric.ed.gov/?id=ED594190
- 96. Aggarwal SK. Cannabis Fear Deconditioning: An Autobiological Marijuana Memoir of a South Asian-Oklahoman Physician-Scientist. Journal of Ethnobiology, 2018 ;38(4):489–503. 10.2993/0278-0771-38.4.489
- 97. Atakan Z. Cannabis, a complex plant: different compounds and different effects on individuals. Therapeutic advances in psychopharmacology. 2012 ;2(6):241–54. 10.1177/2F2045125312457586
- 98. Sill M. The future of the CBD industry in 2022 and beyond. Forbes Business Council, 2021 . https://www.forbes.com/sites/forbesbusinesscouncil/2021/10/21/the-future-of-the-cbd-industry-in-2022-and-beyond/?sh=4b15803425fd
- 99. Velayanikal M. Start-ups search for a pot of gold in ayurvedic cannabinoids. Live Mint, 2021 . https://www.livemint.com/news/india/startups-search-for-a-pot-of-gold-in-ayurvedic-cannabinoids-11615134175116.html
- 100. Narayanan J. ‘Great to see a misunderstood plant in positive light’: The rise of hemp and its by-products in India. The Indian Express, 2022 . https://indianexpress.com/article/lifestyle/food-wine/fssai-hemp-plant-seeds-food-source-regulation-7637371/
- 101. Joshi D, Rathore BS. Women Substance Abuse a Rising Problem in India. The International Journal of Indian Psychology, 2017;4(3):9. http://www.ijip.in/
- 102. Humeniuk RE, Henry-Edwards S, Ali RL, Poznyak V, Monteiro M. The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST): Manual for use in primary care. World Health Organization, Geneva. 2010. https://www.who.int/management-of-substance-use/assist
- 103. World Health Organization. International Statistical Classification of Diseases and related Health Problems; Tenth revision, 2nd ed. 2004. https://apps.who.int/iris/handle/10665/42980
- 104. Budney AJ. Are specific dependence criteria necessary for different substances: how can research on cannabis inform this issue? Addiction, 2006 ;101:125–133. 10.1111/j.1360-0443.2006.01582.x.
- 105. Earleywine M., Luba R., Slavin M. N., Farmer S., Loflin M. (2016). Don’t wake and bake: morning use predicts cannabis problems. Addiction Research & Theory, 24(5), 426–430. http://dx.doi.org/10.1080/16066359.2016.1177027
- 106. Terry P, Wright KA, Terry P, Wright KA, Cochrane R. Factors contributing to changes in frequency of cannabis consumption by cannabis users in England: A structured interview study. Addiction Research & Theory, 2007 ;15(1):113–9. 10.1080/16066350601012681
- 107. Timberlake DS. A comparison of drug use and dependence between blunt smokers and other cannabis users. Substance Use & Misuse, 2009 ;44(3):401–15. 10.1080/10826080802347651
- 108. Hall WD, Lynskey M. Is cannabis a gateway drug? Testing hypotheses about the relationship between cannabis use and the use of other illicit drugs. Drug and Alcohol Review, 2005 ;24(1):39–48. 10.1080/09595230500126698
- 109. Walsh H, Hindocha C, Duaso M. Commentary on Popova et al.(2017): Co-used and co-administered tobacco and cannabis (marijuana) require further investigation. Addiction, 2017 ;112(10):1830–1. 10.1111/add.13972
- 110. Best D, Best D, Gross S, Best D, Gross S, Manning V, Best D, Gross S, Manning V, Gossop M, Best D. Cannabis use in adolescents: the impact of risk and protective factors and social functioning. Drug and Alcohol Review, 2005 ;24(6):483–8. 10.1080/09595230500292920
- 111. Borca G, Rabaglietti E, Roggero A, Keller P, Haak E, Begotti T. Personal values as a mediator of relations between perceived parental support and control and youth substance use. Substance Use & Misuse, 2017 ;52(12):1589–601. 10.1080/10826084.2017.1293103
- 112. King KA, Vidourek RA, Merianos AL, Bartsch LA. Predictors of recent marijuana use and past year marijuana use among a national sample of Hispanic youth. Substance Use & Misuse, 2015 ;50(11):1395–405. 10.3109/10826084.2015.1013136
- 113. Merikangas KR, Li JJ, Stipelman B, Yu K, Fucito L, Swendsen J, Zhang H. The familial aggregation of cannabis use disorders. Addiction, 2009 ;104(4):622–9. 10.1111/j.1360-0443.2008.02468.x
- 114. Richter L, Pugh BS, Ball SA. Assessing the risk of marijuana use disorder among adolescents and adults who use marijuana. The American Journal of Drug and Alcohol Abuse, 2017 ;43(3):247–60. http://dx.doi.org/10.3109/00952990.2016.1164711
- 115. Houck JM, Bryan AD, Feldstein Ewing SW. Functional connectivity and cannabis use in high-risk adolescents. The American Journal of Drug and Alcohol Abuse, 2013 ;39(6):414–23. 10.3109/00952990.2013.837914
- 116. Swift W, Coffey C, Carlin JB, Degenhardt L, Calabria B, Patton GC. Are adolescents who moderate their cannabis use at lower risk of later regular and dependent cannabis use?. Addiction, 2009 May;104(5):806–14. 10.1111/j.1360-0443.2009.02534.x
- 117. Hayatbakhsh MR, Najman JM, Bor W, O’Callaghan MJ, Williams GM. Multiple risk factor model predicting cannabis use and use disorders: a longitudinal study. The American Journal of Drug and Alcohol Abuse, 2009 ;35(6):399–407. 10.3109/00952990903353415
- 118. Hines LA, Morley KI, Strang J, Agrawal A, Nelson EC, Statham D, Martin NG, Lynskey MT. The association between speed of transition from initiation to subsequent use of cannabis and later problematic cannabis use, abuse and dependence. Addiction, 2015 ;110(8):1311–20. 10.1111/add.12963
- 119. Ellickson PL, D’Amico EJ, Collins RL, Klein DJ. Marijuana use and later problems: When frequency of recent use explains age of initiation effects (and when it does not). Substance Use & Misuse, 2005 ;40(3):343–59. 10.1081/JA-200049356