Introduction
An attractive balanced smile is a prime objective of modern orthodontic therapy. As Wylie stated: “The goal of orthodontic treatment should be the attainment of the best possible esthetic result, dentally and facially. However, he emphasized that these qualities should be judged not only in repose but in animation as well. It was in 1958 when Frush and Fisher proposed the term smiling line, in which they mentioned that there should be a harmony between the curvature of the incisal edges of the maxillary anterior teeth and the curvature of the upper border of the lower lip. As years passed by, esthetics started to gain more importance apart from function. It is the orthodontist’s ability to recognize the positive factor for smile esthetic enhancement and to plan treatment accordingly., In general, a flat smile arc leads to decreased smile esthetics. The cause can be due to the intrusion of incisors or extrusion of canines or vice versa. Conventional orthodontic alignment of the maxillary and mandibular arches can also result in the loss of the curvature of the maxillary incisors relative to the lower lip curvature. Hence, it is important to assess and visualize the incisor–smile arc relationship and place brackets accordingly so as to extrude the maxillary incisors or intrude the maxillary canines. Positioning the bracket occlusally or gingivally can certainly lead to intrusion or extrusion of the tooth. Therefore, idealization of the arch can be brought about by altering the bracket position.
To meet the above-mentioned objectives, in the present study, the effects of the MBT Bracket Position in patients with ideal smile arc in the pretreatment and postalignment phases have been evaluated. Following this, the efficacy of modifying the MBT anterior bracket position among patients with flat smile arc in pretreatment and postalignment phases has also been performed. Following this, the evaluation and comparison of the tip, torque, and intercanine width dimension in pretreatment and postalignment phases in both smile arcs have been carried out and the results are reported.
Materials and Methods
This study was conducted by evaluating records of patients undergoing orthodontic treatment in the Department of Orthodontics and Dentofacial Orthopaedics. After obtaining the approval from the “Institutional Review Board,” the patients were explained about the study and a written informed consent was obtained from those who voluntarily participated in this study. The methodology and protocols involved for the selection criteria of the patients has been outlined below.
Inclusion Criteria
Both males and females of the age group between 15 and 24 years.
Absence of any relevant medical history.
Absence of any genetic disorder.
No previous orthodontic treatment.
Dentoalveolar Angle’s Class I malocclusion.
Possessing normal size and shape of the teeth.
Minimal or absence of crowding.
All the study subjects were treated with preadjusted edgewise appliance, MBT prescription (0.022 slot, American orthodontics, USA).
Exclusion Criteria
Patients with previous history of orthodontic treatment.
Patients with syndrome.
Methodology Involved
The patients were divided into two groups. Group A consisted of 15 patients with ideal smile arc whereas group B comprised of 15 patients with flat smile arc.
Pretreatment and postalignment upper impressions of all the patients were taken using alginate impression material and casts were poured immediately with orthocal stone to avoid error caused during impression shrinkage.
Pretreatment and postalignment panoramic radiographs of all the patients were taken using PLANMECA (PROMAX Oy 00880, Finland).
All panoramic radiographs were taken under standard conditions with a cephalostat, by keeping the clinical Frankfort horizontal plane parallel to floor and the facial midline plane in a vertical position.-
Films were exposed at 60-72 kV with 1-16 mA, where a filter of 2.5 mm aluminum equivalent was used.
Tip values of upper anteriors (mesiodistal inclination) were evaluated from pretreatment and postalignment panoramic radiographs which were traced by taking orbital floor as the reference plane.
Torque values of upper anterior were derived from pretreatment and postalignment study models using torque angulation device.
The study cast was stabilized on an immobile surveyor table to avoid error during torque evaluation.
The horizontal occlusal line was set parallel to the granite platform of the torque angulation device. The horizontal line is an imaginary line connecting right and left molar buccal cusp tips, midpoint of right and left central incisor (Incisal edge). The crown inclination was recorded with the help of the moving torque fine adjustment knob until the blade was well adapted to the Long Axis (LA) point and the measurements were recorded which were displayed on the screen.
Intercanine width was also evaluated from pretreatment and postalignment study models using a Digital Vernier caliper (precision of 0.01 mm, Figures 1 and 2).
The subjects were photographed with posed smiles (most repeatable) after seating the patient in the natural head position using a cephalostat., Ear rods of the cephalostat were used to stabilize the patient’s head.
Photographs were taken in the same environment with same lighting conditions by using NIKON DSLR-D70S camera. The camera was fixed with a tripod stand at a distance of 50 cm from the cephalostat.
All the photographs that were taken at 2 intervals were distributed to 10 (7 females and 3 males) lay persons for evaluation (Figure 3a–d).
A 10-point visual analogue bar scale was created for scoring. All the evaluators were asked to score the smile according to their preference. The visual analogue scale was converted later into grades from 0 to 10, the least attractive being 0 and the most attractive was given a score of 10.
Extra oral smile photographs were used for the evaluation of extrusion or intrusion of the upper anteriors by designing an ideal smile arc with teeth in its correct position. Following this, the distance from the incisal edges of the specific teeth to that of the created one was measured using “Smile Designer Pro Software” (version 1.1, Toronto, Canada).
Once evaluation of the intrusion and extrusion was done, brackets were bonded according to the criteria for correction of flat smile arc. Archwire were placed in the following sequence: 0.016 Niti, 0.016 × 0.022 Niti, 0.017 × 0.025 Niti, 0.019 × 0.025 Niti, and 0.021 × 0.025 Niti with individual ligation.
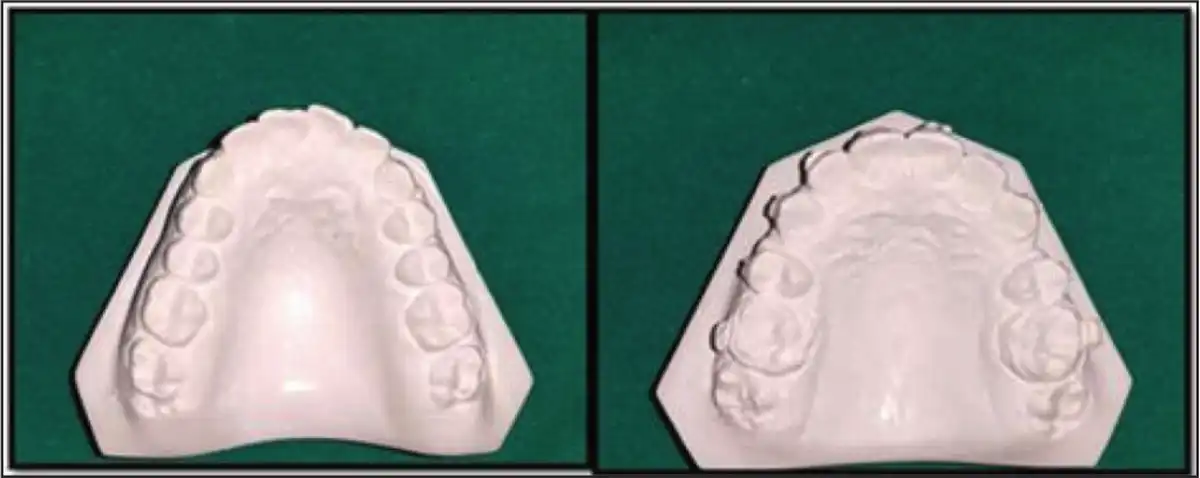
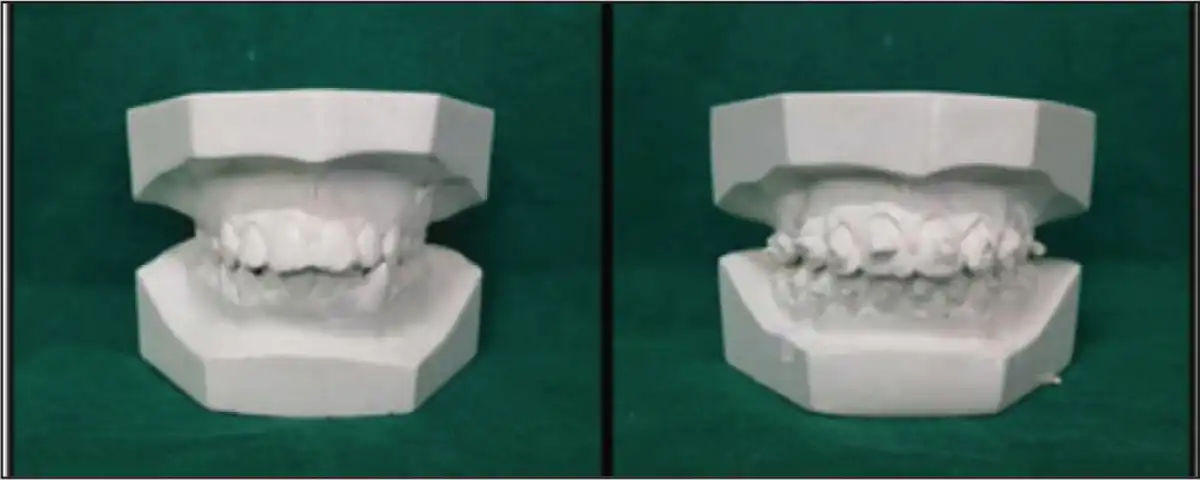
Comparison of Pretreatment and Postalignment Maxillary Study Cast Model: Group A (Occlusal View)
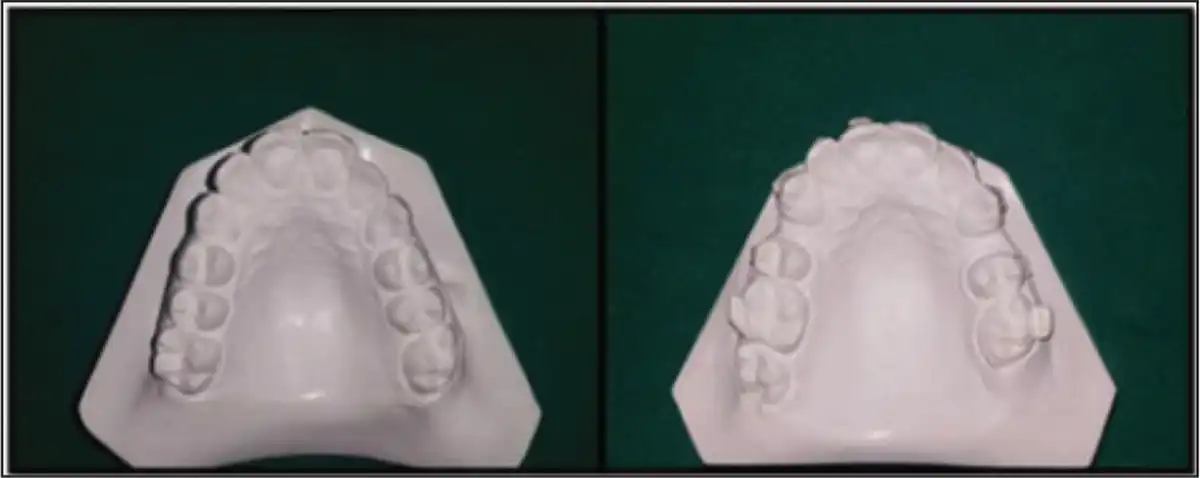
Comparison of Pretreatment and Postalignment Maxillary Study Cast Model: Group B (Occlusal View)
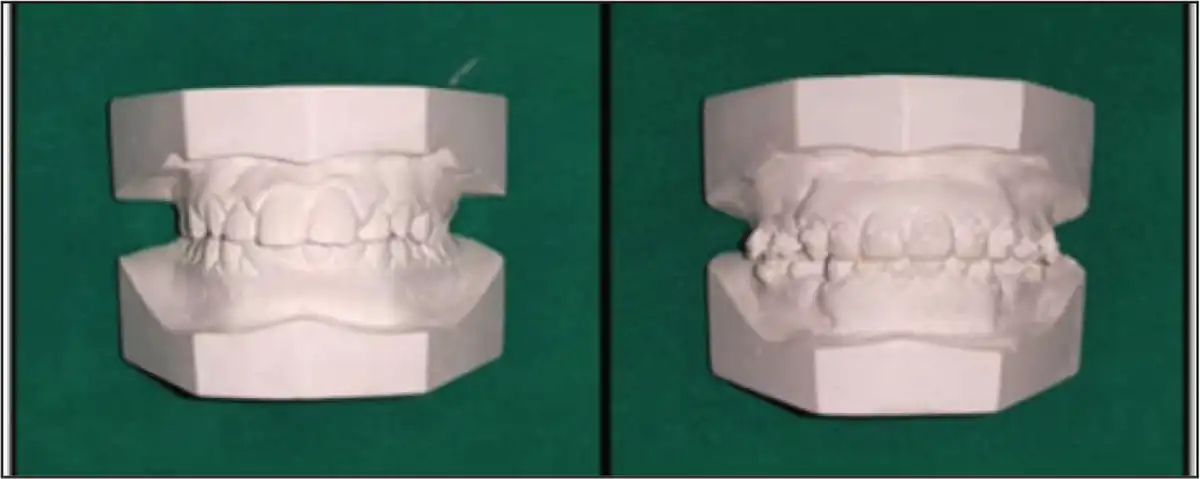
Comparison of Pretreatment and Postalignment Study Cast Model: Group A
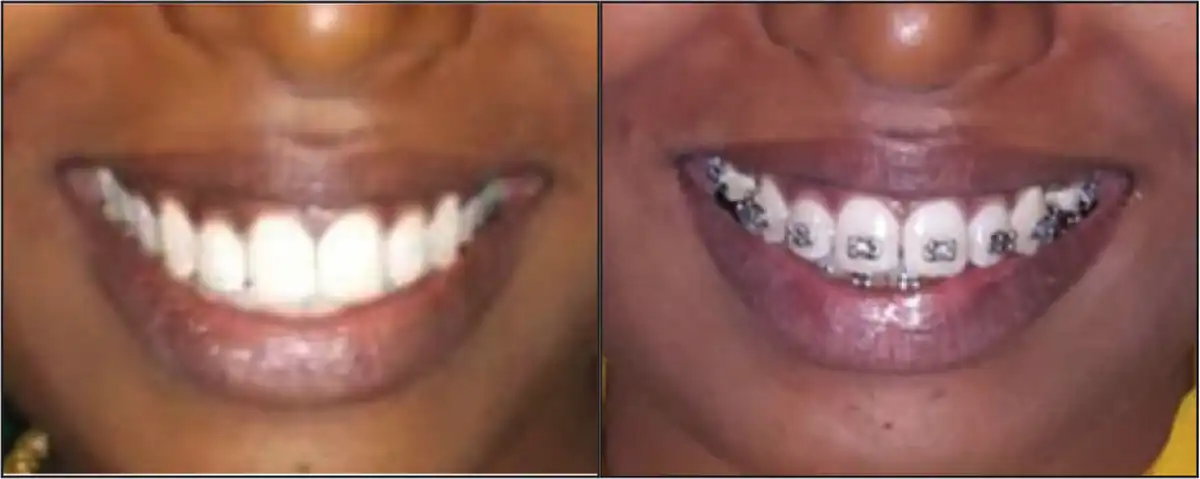
Comparison of Pretreatment and Postalignment Photograph: Group A
Reliability of Measurements
Both radiographic tracing and bracket positioning was done by the same investigator to avoid interoperator error. Smile photographs were also taken by a single observer. No statistically significant variations were found between these readings; hence, the first trial values were used for the statistical analysis.
Comparison of Pretreatment and Postalignment Study Cast Model: Group B

Comparison of Pretreatment and Postalignment Photograph: Group B
Statistics
Paired student t test was performed to find the level of significance in tip and torque values for pretreatment and postalignment phases in both the groups. Wilcoxon signed ranks test was used to determine the statistically significant changes observed in torque in relation to all the maxillary anteriors. Mann–Whitney test was carried out to find the level of significance in mean difference in intercanine width and visual analogue scale for both the groups. All the statistical analysis was performed using the Statistical Package for Social Sciences (SPSS, version 16.0; SPSS Inc., USA).
Results
30 subjects who were divided into 2 groups on the basis of their smile arc were photographed with posed smile in frontal view. A 10-point visual analogue scale was used to record the improvement in the smile arc. Pretreatment and postalignment maxillary study cast models were taken for the evaluation of the torque of maxillary anteriors and intercanine width. Pretreatment and postalignment panoramic X-rays were taken for the evaluation of the tip of maxillary anteriors. All values of the variables were obtained manually and entered into an excel spreadsheet. The mean scores obtained for both groups under different variables were then calculated and tabulated in the following manner for further statistical analysis.
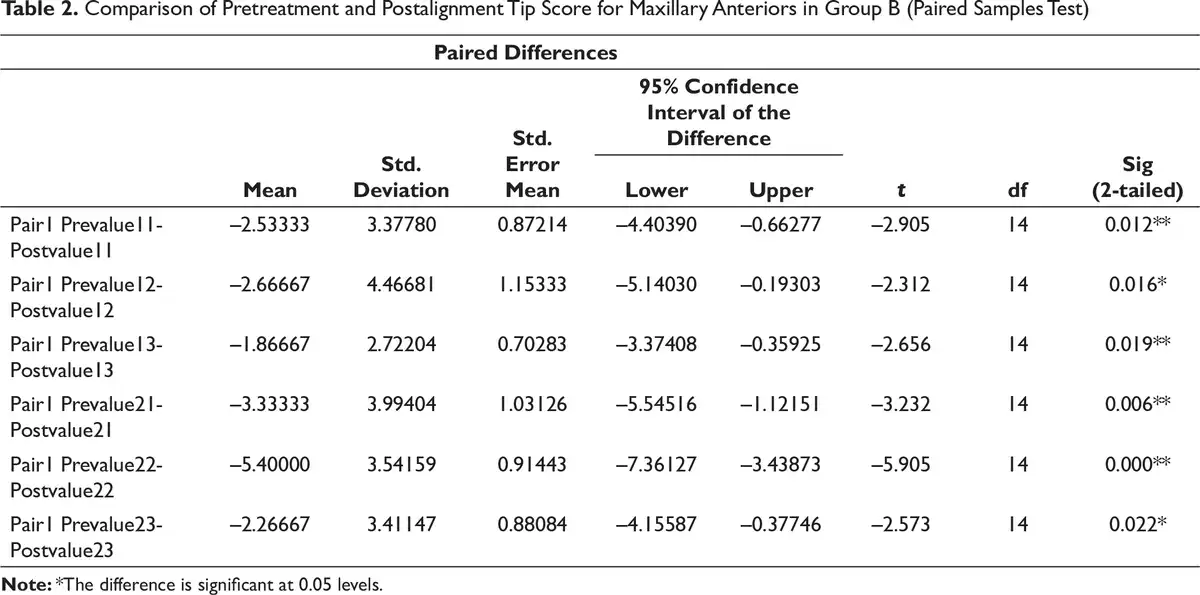
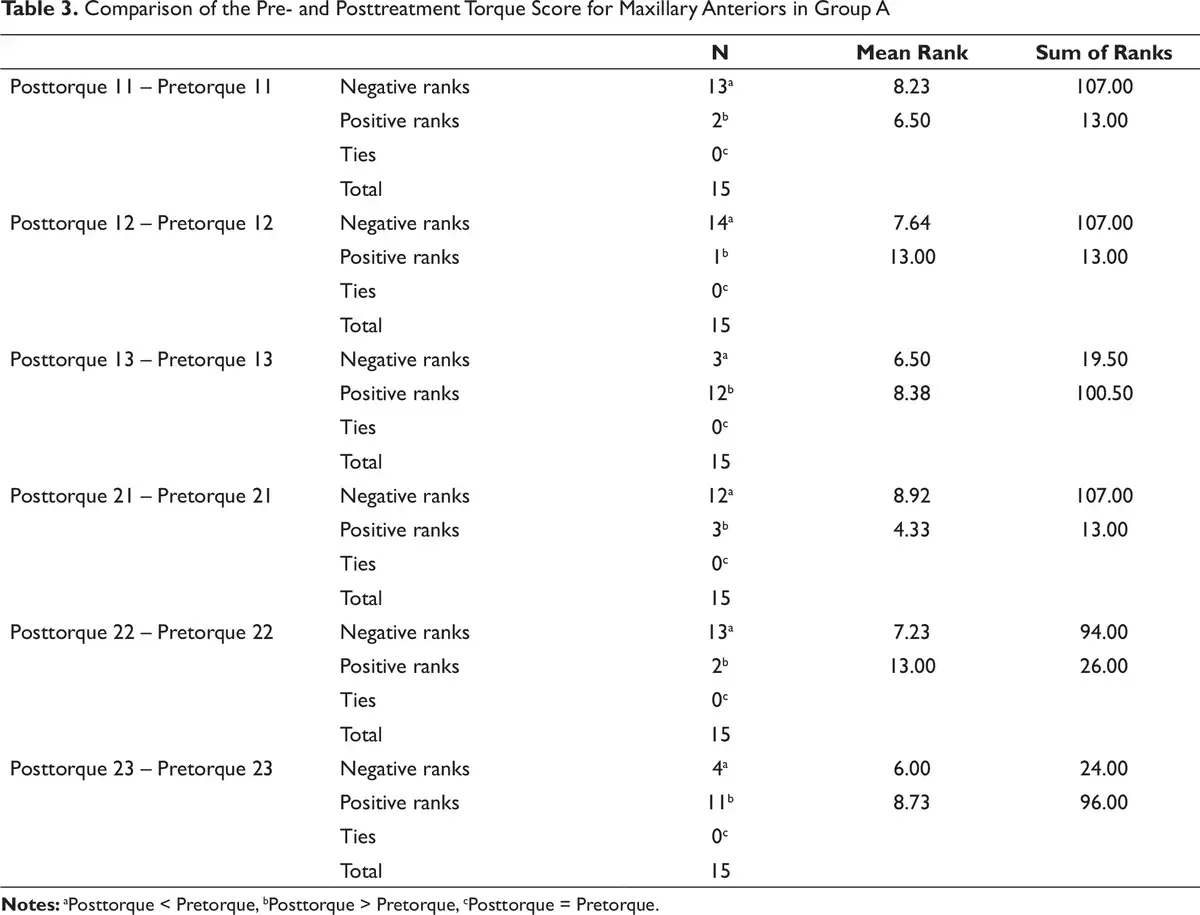
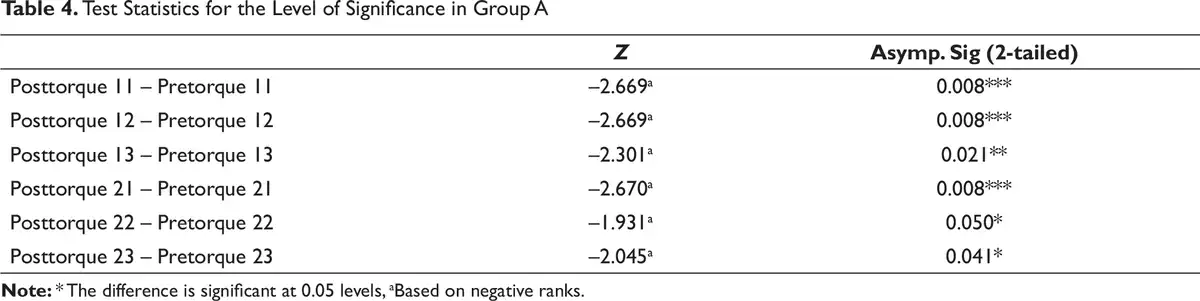
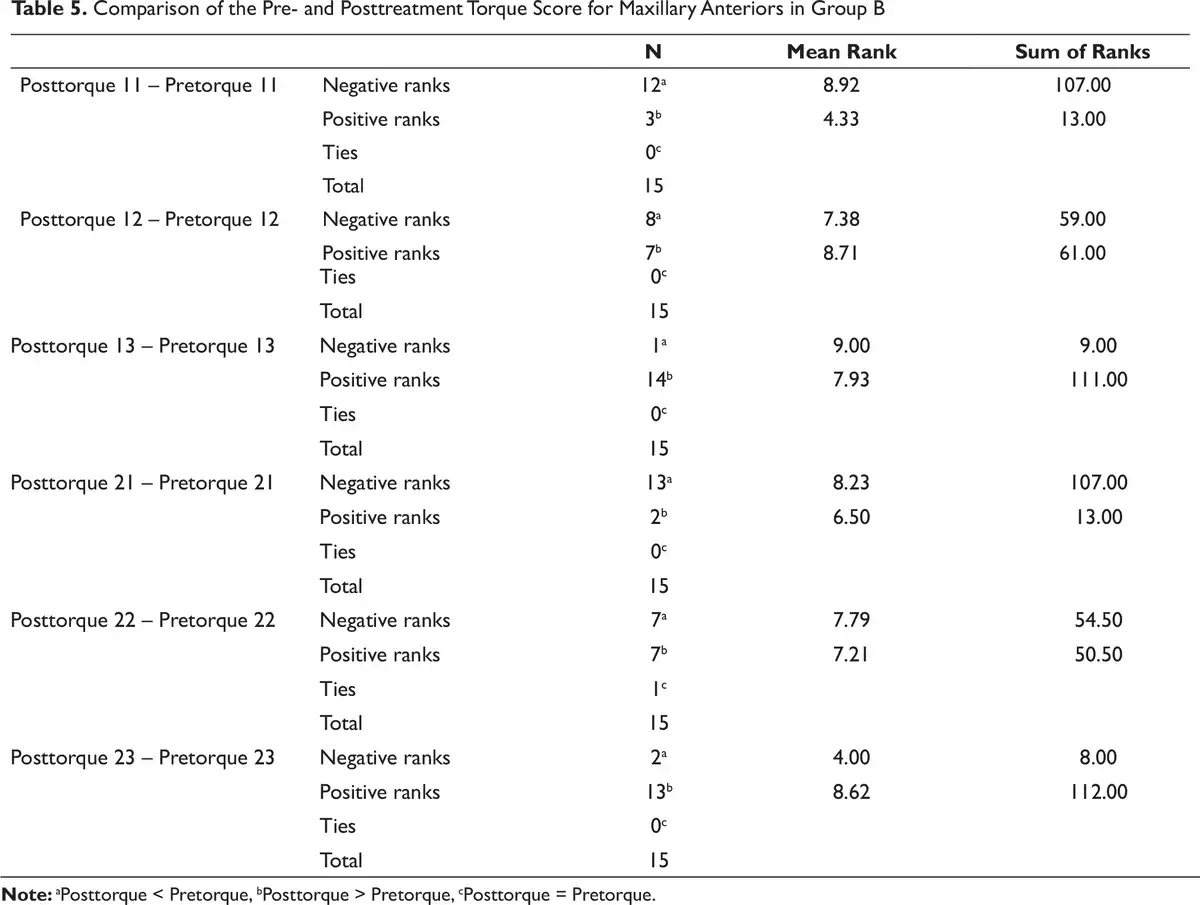
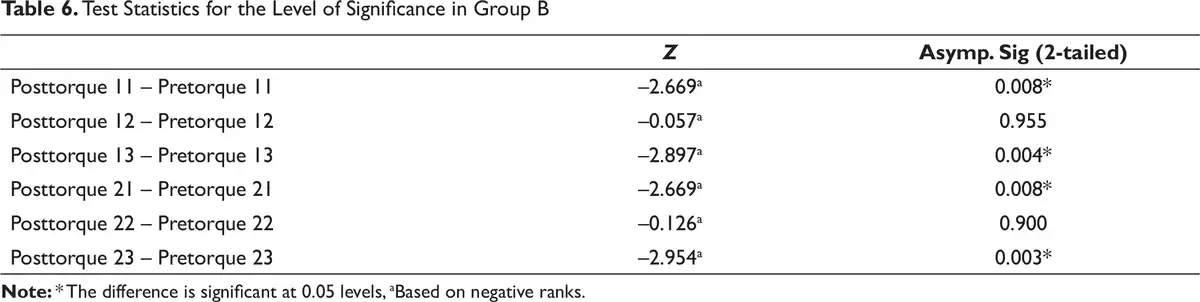
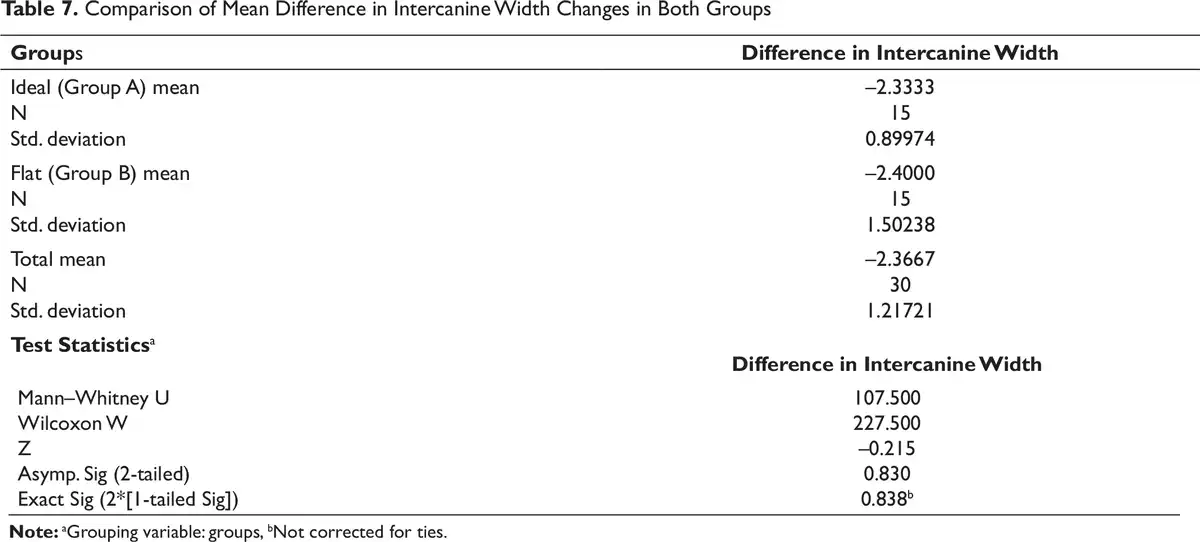
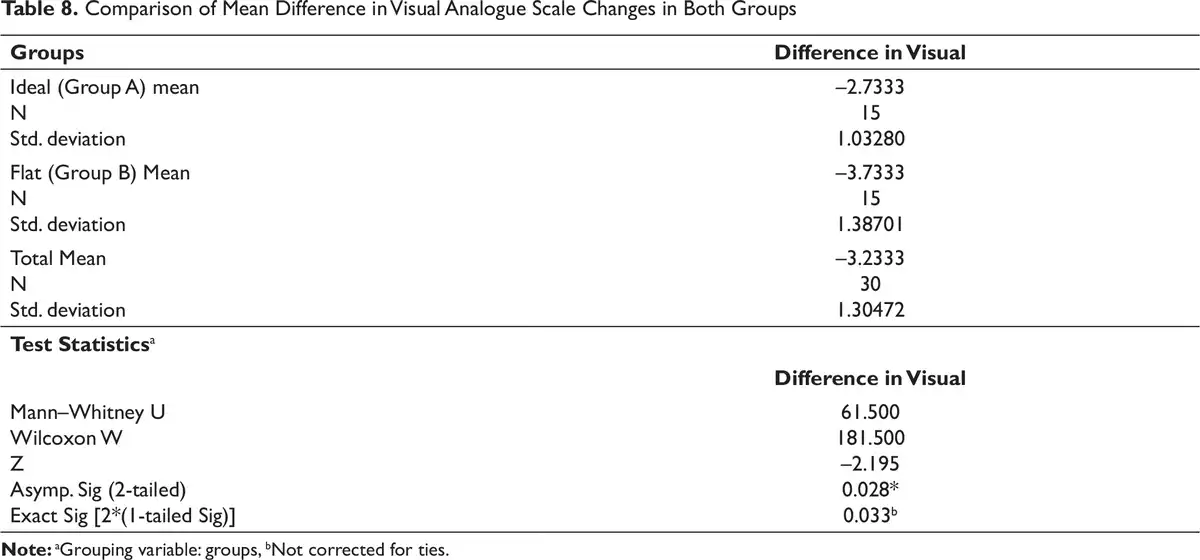
Paired student t test was performed to find out the level of significance in tip and torque values for pretreatment and postalignment phases in both the groups. The results showed that group A has possessed a statistically significant difference for the tip values in relation to maxillary anteriors except maxillary left canines (Table 1), whereas for group B statistically significant difference was observed for the tip values in relation to all the maxillary anteriors (Table 2). Wilcoxon signed ranks test for group A indicated that statistically significant changes were observed in torque in relation to all the maxillary anteriors (Tables 3 and 4). Similarly, Wilcoxon signed ranks test for group B also indicated that statistically significant change was found in relation to both right and left maxillary incisors and canines. However, there was no significant change observed in relation to maxillary right and left lateral incisors (Tables 5 and 6). Mann–Whitney test was carried out to find the level of significance in mean difference in intercanine width (Table 7) and visual analogue scale (Table 8) for both the groups. All ratings of the visual analogue scale were converted to values and tabulated for statistical analysis. From the Mann–Whitney results, it was found that while the mean difference in intercanine yielded not much statistical significance, the mean difference in visual analogue scale possessed a statistically significant difference between the groups. This showed that there was a significant change in group B when compared with the results achieved in group A.

Discussion
In the present clinical study, patients were selected mainly on a single dental malocclusion just to avoid many variables, since there are variations in the structure of a smile according to age, sex, and race. The esthetics of subjects was restricted within the age group of 15 to 24 years. Studies have shown that people in this age group seek orthodontic treatment because the desire for looking good among the peers is generally increased. Evaluation of the relative intrusion or extrusion of the maxillary anteriors with proper standardization was done using Smile Designer Pro Software. Posed smile photographs were used to visualize the improvement in smile arc. Recently, the visual analogue scale gained popularity for measuring subtle changes in dental and facial attractiveness where moderately to high correlation has been reported.- In the present study, the visual analogue scale allowed a simple and rapid method for evaluating the changes achieved by bracket position modification. Moore et al found that there was no significant difference in smile esthetics perception between male and female judges. Hence, the gender of the evaluators was not considered significantly in perceiving smiles. Evaluation of mean scores of the groups indicated that changes achieved in group B were statistically significant than group A. This agrees with the statement by Maganzini et al that “smile esthetics improves regardless of the initial severity of the malocclusion provided proper bracket position modifications are done.
Tip and Its Influence on Smile
In group A, all the tip values indicated that there was distal tipping of maxillary anteriors which were statistically significant except for maxillary left canines (Table 1). Generally during the aligning stage, lacebacks are given to prevent mesial tipping of the canine and to overcome proclination of anteriors caused due to expression of the inbuilt tip in the canine bracket. However, in the present study, maxillary left canines did not express more distal tipping as observed in the anterior teeth. The reason could be due to improper activation or reduced activation of lacebacks. Also, the maxillary left canines are located farther from the operator’s view, and hence, errors in activation could have contributed to this altered tip values. Khambay et al has proved that there is a large variation in the activation of lacebacks between two time points. In group B, tip values revealed that all the maxillary anteriors had significant distal tipping (Table 2). This would have been occurred due to altered bracket positioning for the correction of the flattened smile arc, ie, incisor brackets were placed mildly gingivally for extrusion and the canine brackets were placed incisally for intrusion or a combination of both.
Torque Expression and Smile Arc
The pretreatment and postalignment torque values were gained from a digital torque angulation device (Table 3). All the maxillary anteriors had positive torque values except in few maxillary canines where negative torque values were observed. The statistically significant torque values obtained for group A proved that the bracket inbuilt torque has been well expressed in all the maxillary anteriors (Table 4). Nevertheless, the torque values observed in group B were found to be statistically significant except for the maxillary lateral incisors because there was an uncontrolled mesiodistal tipping which would have hampered the complete torque expression in the lateral incisor bracket (Tables 5 and 6). Major change in the torque for maxillary canine was due to simultaneous intrusion and distal tipping which would have pushed the roots of maxillary canine into the cancellous bone leading to complete torque expression of the canine. Raghuraj et al evaluated the efficacy of tip and torque of MBT brackets in orthodontic treated individuals and concluded that torque was overexpressed in maxillary canines and lateral incisors, whereas it was underexpressed in maxillary central incisors. Contrary to this, in our study we found that torque was well expressed both in the maxillary central incisors and canines.
Intercanine Width and Smile Arc
Measurements obtained for the intercanine width and visual analogue scale from the maxillary study casts showed increased width in flat smile arc group when compared to ideal smile arc group which was not significant (Tables 7 and 8). This proved that intercanine width dimensions increase regardless of bracket positioning. The main reason for increase in intercanine width was possibly because of minor lateral movement of the canine as they moved distally into the premolar extraction space as reported by Gianelly. Ackermann et al had suggested that broader the archform, the lesser will be the curvature of the maxillary anteriors leading to a flat smile arc. In the present study, it was observed that by modifying the bracket position considerable changes in the teeth position can be accomplished without altering the balance between the esthetic smile arc and functional occlusion. Many studies have concluded that normal orthodontic treatment leads to flatter smiles. However, in this study it was proved that standard bracket positioning does not lead to flatter smile until postalignment stage. Castellonas et al have recently introduced a new chart for bracket placement based on the concept of smile arc protection where they claim that smile arc flattening can be prevented if brackets are placed according to the newly developed bracket placement chart. Accordingly, the present study proved that ideal smile arc can be achieved in flat smile arc cases by modifying bracket position, and hence, it can be inferred that bracket positioning plays a vital role in achieving an ideal smile arc.
Conclusion
Understanding the relationship between smile and malocclusion is important in orthodontic treatment planning. Though many variables can be considered, intrusion/extrusion of the maxillary anteriors and their relationship with lower lip plays a crucial role in improving overall smile esthetics. In this prospective clinical study, the included 30 patients were divided into 2 groups of 15 each having ideal smile arc and flat smile arc. Smile evaluation was performed using smile photographs, tip was assessed using panoramic radiographs, and torque and intercanine width changes were evaluated using study casts at the end of alignment phase in both the groups. Conclusions of the study revealed:
Ideal smile arc was maintained in ideal smile arc group at the end of postalignment stage.
Change in tip value of all the maxillary anteriors was significant except for maxillary left canines. Postalignment torque expression was significant in all the maxillary anteriors.
The smile arc achieved was ideal in flat smile arc group at the end of postalignment stage.
In flat smile arc group, significant mesiodistal tipping was observed in all maxillary anteriors. Significant torque expression was also observed in all maxillary anteriors except maxillary lateral incisors.
Intercanine width dimension was increased more in flat smile arc group when compared to ideal smile arc group. Overall a simple modification in bracket positioning might establish an esthetically pleasing smile arc in patients with pretreatment flat smile arc.
L. Karthik
https://orcid.org/0000-0002-3854-6004
References
- 1. Wendell L. Wylie. The mandibular incisor: its role in facial esthetics. Angle Orthod. 1955;25(1):32–41.
- 2. Frush JP, Fisher RD. The dynesthetic interpretation of the dentogenic concept. J Prodthet Dent. 1958;8:558.
- 3. Sarver DM, Ackerman MB. Dynamic smile visualization and quantification: part 1. Evolution of the concept and dynamic records for smile capture. Am J Orthod Dentofacial Orthop. 2003;124:4–12.
- 4. Sarver DM, Ackerman MB. Dynamic smile visualization and quantification: part 2. Smile analysis and treatment strategies. Am J Orthod Dentofacial Orthop. 2003;124:116–127.
- 5. Sarver DM. The importance of incisor positioning in the esthetic smile: the smile arc. Am J Orthod Dentofacial Orthop. 2001;120(2):98–111.
- 6. McKee IW, Williamson PC, Lam EW, Heo G, Glover KE, Major PW. The accuracy of 4 panoramic units in the projection of mesiodistal tooth angulations. Am J Orthod Dentofacial Orthop. 2002;121:166–175.
- 7. Kannabiran P, Gnanasagar J, Mahendra L. The crown angulations and inclinations in Dravidian population with normal occlusion. IJDR. 2012;23(1):53–58.
- 8. McKee IW, Williamson PC, Lam EW, Heo G, Glover KE, Major PW. The effect of vertical and horizontal head positioning in panoramic radiography on mesiodistal tooth angulations. Angle Orthod. 2001;71:442–451.
- 9. De Almeida-Pedrin RR, Pinzan A, de Almeida RR, Ursi W, de Almeida MR. Panoramic evaluation of mesiodistal axial inclinations of maxillary anterior teeth in orthodontically treated subjects. Am J Orthod Dentofacial Orthop. 2006;130(1):56–60.
- 10. Hegde T, Dattada H, Jaiswal RK. AN Avant-garde indirect bonding technique for lingual orthodontics using the first complete digital “TAD” (torque angulation device), & “BPD” (bracket positioning device). J Indian Orthod Soc. 2010;44:9–16.
- 11. Raghuraj MB, Amin V, Husain A, Mascarenhas R, Shetty S. Evaluation of efficacy of the MBT appliance in expressing inbuilt tip and torque values: using torque angulation device. J Orthod Res. 2014;2:135–141.
- 12. Ackerman MB, Ackerman JL. Smile analysis and design in the digital era. J Clin Orthod. 2002;36(4):221–236.
- 13. Sarver DM, Ackerman JL. Orthodontics about face: the re-emergence of the esthetic paradigm. Am J Orthod Dentofacial Orthop. 2000;117(5):575–576.
- 14. Phillips C, Tulloch C, Dann C. Rating of facial attractiveness. Community Dent Oral Epidemiol. 1992;20(4):214–220.
- 15. Kokich VO, Asuman Kiyak H, Shapiro PA. Comparing the perception of dentists and lay people to altered dental esthetics. J Esthet Restorative Dent. 1999;11(6):311–324.
- 16. Maple JR, Vig KW, Beck FM, Larsen PE, Shanker S. A comparison of providers’ and consumers’ perceptions of facial-profile attractiveness. Am J Orthod Dentofacial Orthop. 2005;128(6):690–696.
- 17. Howells DJ, Shaw WC. The validity and reliability of ratings of dental and facial attractiveness for epidemiologic use. Am J Orthod. 1985;88(5): 402–408.
- 18. Moore T, Southard KA, Casko JS, Qian F, Southard TE. Buccal corridors and smile esthetics. Am J Orthod Dentofacial Orthopedics. 2005;127(2):208–213.
- 19. Maganzini AL, Schroetter SB, Freeman K. Improvement in smile esthetics following orthodontic treatment: a retrospective study utilizing standardized smile analysis. Angle Orthod. 2013;84(3):492–499.
- 20. Khambay BS, McHugh S, Millett DT. Magnitude of reproducibility of force generated by clinicians during laceback placement. J Orthod. 2006;33(4):270–275.
- 21. Andrews LF. The six keys to normal occlusion. Am J Orthod. 1972;62(3):296–309.
- 22. Gianelly AA. Arch width after extraction and non-extraction treatment. Am J Orthod Dentofacial Orthop. 2003;1123(1):25–28.
- 23. Ackerman J, Ackerman MB, Brensinger CM, Landis JR. A morphometric analysis of the posed smile. Clin Orthod Res. 1998;1:2–11.
- 24. Zachrisson BU. Esthetic factors involved in anterior tooth display and the smile; vertical dimension. J Clin Orthod. 1998;32:432–445.
- 25. CE F. A new table to guide bracket placement based on concept of “smile arc protection”.