The COVID-19 pandemic has impacted people’s lives immensely. Vaccination was seen as the most efficient way to stop the spread of the coronavirus; however, not everyone was willing to get a COVID-19 vaccine (; ; ). Many countries have installed policies at various points of the pandemic that were designed to curb the spread of the virus while encouraging citizens to get vaccinated, for example through a COVID-19 pass that one needed for access to public places. Citizens have perceived many of these policies as a form of coercion to get vaccinated, and conspiracy theories about the vaccines have spread rapidly (an “infodemic”; ). Moreover, the vaccination campaigns have increased polarization between vaccinated and unvaccinated people (; ; ; ). For instance, vaccinated people have blamed unvaccinated people for being responsible for prolonging the pandemic, leading them to support more restrictive policies toward unvaccinated people (); at the same time, many of these restrictive policies may be perceived as unfair and exclusionary by unvaccinated people. The present research examines what role conspiracy theories play in these processes, and how polarization is related to people’s vaccination status.
Conspiracy mentality is conceptualized as a general predisposition to interpret many events in the world as being caused by conspiracies, while specific conspiracy beliefs pertain to specific societal events (e.g. the pandemic) as being caused by a conspiracy (). Those conspiracy theories are usually unsubstantiated. Although these constructs are highly correlated, and are even used interchangeably in many studies, their more specific effects may differ (e.g. ). One noteworthy difference is that conspiracy mentality is more relatively stable over time while specific conspiracy beliefs are more malleable by situational factors (e.g. ; ; ).
Previous research has revealed that conspiracy beliefs predict reduced COVID-19 preventive behaviors, such as keeping social distance and wearing face masks (; ; ; ; ) and reduced COVID-19 vaccination intentions (; ; ; ; ). Conspiracy beliefs may even discourage families or friends from getting vaccinated (; see also ). However, much is still unclear about how these conspiracy beliefs have inspired polarization across societal groups throughout the vaccination campaign. Many media sources have reported tensions between vaccinated and unvaccinated people (; ; ; ). What role do conspiracy beliefs play in such polarization of people with a different vaccination status? To address these questions, we have examined the associations between perceived vaccination coercion, conspiracy beliefs about the COVID-19 vaccines, and polarization in three countries: the US, the UK, and China. Moreover, we have collected data to balance the number of vaccinated and unvaccinated citizens in our samples, to investigate the relationship of vaccination status with these variables.
Conspiracy beliefs, vaccination hesitancy and vaccination status
As some vaccination policies have exerted pressure, particularly on people who were hesitant to get vaccinated, many of them might have felt some level of coercion to get vaccinated. This pressure may have stimulated people to justify their decision not to get vaccinated, making them sensitive to motivated reasoning processes (). Notably, the discrepancy between vaccination hesitancy and social norms of getting vaccinated during the pandemic may have prompted feelings of cognitive dissonance, stimulating motivated reasoning (; ; ).
Conspiracy beliefs can be part of such a motivated reasoning process, to serve ideological and psychological needs () and political interests (). Motivated by the goal of not being vaccinated, people may become increasingly susceptible to misinformation (e.g. “vaccines are unsafe”) and conspiracy theories (). For instance, found that conspiracy beliefs negatively predicted inoculation with the COVID-19 vaccines. As such, conspiracy beliefs help to legitimize people’s behavior that is perceived as counter-normative in the broader society (). In a longitudinal study, found that vaccination hesitancy shapes increased conspiracy beliefs over time. Moreover, perceived vaccination coercion is likely to increase feelings of powerlessness and uncontrollability among vaccination-hesitant people. Such feelings of uncontrollability and lack of power are associated with increased conspiracy beliefs (; ; ; ). Based on these arguments, we hypothesize that unvaccinated people experience more vaccination coercion (Hypothesis 1a) and endorse stronger conspiracy beliefs about the COVID-19 vaccines (Hypothesis 1b).
While specific (e.g. vaccination) conspiracy beliefs are relevant in specific situations (e.g. a pandemic), conspiracy mentality indicates people’s general susceptibility to these conspiracy theories. The current study examined conspiracy mentality and COVID-19 vaccine conspiracy beliefs among groups of vaccinated and unvaccinated people. This actual vaccination status meaningfully extends research on vaccination intention given that intentions and actual behaviors do not always converge (e.g. ). For example, many people may be vaccination hesitant yet get vaccinated; likewise, some people may not be vaccination hesitant yet do not get vaccinated due to medical reasons. In light of the many studies that have found a relationship between vaccination hesitancy and conspiracy beliefs (; ; ; ; ), and taking into account that vaccination pass policies would limit the opportunities of only unvaccinated people, it stands to reason that unvaccinated people have a higher level of conspiracy mentality and experience more vaccination coercion. Hence, we hypothesize that conspiracy mentality is associated with perceived vaccination coercion (Hypothesis 2).
Vaccination status and polarization
Vaccination status has divided people into two groups during the COVID-19 pandemic, and values about vaccination became polarized in both groups (; ; ; ). Polarization is reflected in a strong conviction in the correctness of one’s beliefs, perceived moral superiority of one’s own values and beliefs, and conflict and hostility toward those who hold different values and beliefs (). In the context of the COVID-19 vaccination campaign, vaccination statuses were particularly salient as a result of policies to reduce the spread of the corona virus. Given that people needed a vaccination pass to get access to public places with colleagues or friends, often it was clear who was vaccinated or not – this unlike other vaccines, where it usually is less clear to people who are and are not vaccinated.
Both vaccinated and unvaccinated people have shown ingroup favoritism, and were polarized in their attitudes and behaviors (). Before the pandemic, researchers noticed that both people who are pro-vaccination and anti-vaccination were polarized in their social media behaviors (e.g. likes, comments; see ). In addition, people are likely to receive information mainly from their “echo-chambers” (), which may increase polarization. Although both groups are likely to be polarized, evidence showed that vaccinated and unvaccinated people may not have polarized to an equal extent. For example, during the COVID-19 pandemic, Twitter conversations about vaccination were highly polarized especially among unvaccinated people (). Therefore, we predicted that unvaccinated people would be more polarized toward vaccinated people than vice versa (Hypothesis 3).
While some vaccination policies may have increased uptake rate, some of these policies also may have stimulated conspiracy beliefs, especially considering that the COVID-19 vaccines are relatively new and have been developed in a short timeframe. To the extent that people experience vaccine policies as coercive, increased conspiracy beliefs about the COVID-19 vaccines might be endorsed to justify people’s vaccination hesitancy (; ). Besides, people tend to expose themselves to information and people that validate their existing beliefs, contributing to group polarization (i.e. echo chambers; ; ; ). Particularly unvaccinated people are likely to experience coercion in the vaccination campaign, however, and believe conspiracy theories that may contribute to polarization. We therefore predicted that perceived vaccination coercion promotes intergroup polarization, and that COVID-19 vaccination conspiracy beliefs mediate this effect. Moreover, we expect that vaccination status would moderate the links of perceived coercion with conspiracy belief and polarization, such that these links are significant and positive particularly among unvaccinated people (Hypothesis 4).
The current study
Considering that policies differ across countries, we have collected data from three countries – the US, the UK, and China. In addition to participants’ perceived coercion to get vaccinated, we also measured people’s perceived coerciveness of policies, operationalized as how coercive people rate a standardized series of policies independent of whether they have been implemented in a particular country (as people may differ in how coercive they rate the same policy). In an exploratory fashion, we compared cultural differences for perceived coerciveness of policies as well.
Method
Participants
Within-country, we planned to compare the difference between vaccinated and unvaccinated people. A sample of 400 participants per country would generate a small to medium effect size (d = 0.28, power = 0.80, α = 0.05) for the within-country analyses. US and UK participants were recruited from Prolific (a platform that provides good data quality; see ), Chinese participants were recruited from Credamo (also a platform with good data quality; see ). The total sample size was 1202 participants, with around 200 vaccinated and 200 unvaccinated participants from China, the UK and the US, respectively (for more information, see Online Supplemental materials Table S1). This study has been ethically approved by the Scientific and Ethical Review Board of the Faculty of Behavior and Movement Sciences (VCWE-S-21-00228[80]) at Vrije University Amsterdam. All the hypotheses were pre-registered on OSF: https://osf.io/4bcd8, Data are available via https://osf.io/gqj2s/.
Procedure
The US and the UK reached a population-wide vaccination rate of 67% and 74%, respectively. China used another way of recording the vaccination rate, which was about 1.61 doses per citizen at the survey time. The data collection process started on October 25th, 2021 and ended on October 29th, 2021. Most citizens from these three countries had relatively little difficulty in getting access to the vaccine, as COVID-19 vaccines were widely available to the public (). With the prescreening function offered by Prolific, we were able to selectively target vaccinated and unvaccinated participants in the UK and US. However, this prescreening information might be lagged, as some participants may have taken the vaccine without updating their information on Prolific. In order to reduce the influence of lagged prescreening, and accurately distinguish between vaccinated and unvaccinated participants in our sample, we designed two separate surveys in each country. In addition, we attached an alternative URL link that participants could choose, leading them to the correct survey based on their real vaccination status. Chinese participants were recruited from Credamo, which does not have the prescreening function. Instead, we indicated our target participants in the survey invitation as well as a question to double-check their vaccination status. Moreover, we randomly inserted an attention check (e.g. “Please choose Totally Disagree for this statement”), and a failed attention check would lead to the exclusion of a participant from the data.
Measures
Perceived vaccination coercion
Perceived vaccination coercion was measured by asking participants to what extent they agreed with the statement “There is a lot of pressure from the government on people to get vaccinated” (“1 = Totally Disagree” to “7 = Totally Agree”).
Perceived coerciveness of policies
We asked participants to what extent they believed three measures are forcing people to get vaccinated (“1 = Not Forcing at All” to “7 = Very Much Forcing”) irrespective of whether those measures actually have been implemented in their country. For example, “Without being vaccinated, some employees are fired” (full scales of all measures can be found in the Online Supplemental materials). Cronbach’s α were αChina = 0.87, αUK = 0.84, and αUS = 0.81 respectively.
Conspiracy mentality
We adopted the five-item measurement designed by , but measured on a seven-point scale (“1 = Totally Disagree” to “7 = Totally Agree”) to be consistent with other measurements, for example “Many important things happen in the world, which the public is never informed about.” Reliability in three countries were αChina = 0.88, αUK = 0.83, and αUS = 0.84 respectively.
Conspiracy beliefs
Conspiracy beliefs were measured by asking participants to what extent they agreed with five conspiracy theories about the COVID-19 vaccines, for example, “The COVID-19 vaccines are used to manipulate citizens.” Participants rated each item on a scale from “1 = Totally Disagree” to “7 = Totally Agree.” The reliability of the conspiracy beliefs measurements in three countries were αChina = 0.83, αUK = 0.94, and αUS = 0.96 respectively.
Polarization
After a short reminder of their vaccination status (“You have decided (not) to get vaccinated”), we measured polarization by asking participants to rate to what extent they agreed (“1 = Totally Disagree” to “7 = Totally Agree”) with nine statements about their personal conviction (e.g. “I believe my decision is the only right one”), moralization (e.g. “It is a moral obligation to promote the COVID-19 vaccine” for vaccinated participants and “It is a moral obligation to reject the COVID-19 vaccine” for unvaccinated participants) and perceived conflict (e.g. “I feel angry with unvaccinated people” for vaccinated participants and “I feel angry with vaccinated people” for unvaccinated people). These three elements are in line with the main aspects of polarization (). The reliability of the polarization measurement in the three countries were αChina = 0.94, αUK = 0.91, and αUS = 0.93 respectively.
Results
To test Hypothesis 1a, Hypothesis 1b, and Hypothesis 3, we conducted a range of two-tailed t-tests between vaccinated and unvaccinated groups within each country. Hypothesis 2 was tested with a correlational analysis. Finally, we tested Hypothesis 4 with structural equation modeling. Age, educational background (1 = primary school, 5 = PhD degree), gender (male = −1, female = 1, others = NA) and political orientation (−50 = left-wing, 50 = right-wing) were included as control variables in the moderated mediation model analysis to avoid alternative explanations with demographic information and political orientation (). As it is difficult to reliably measure political orientation in China, this variable was not measured among Chinese participants. As polarization is a multifaceted concept, we treated it as a latent variable. The structural equation model was analyzed with the R package “Lavaan” (). Comparison analyses within-country were conducted with Jamovi (Version 1.6).
Differences between vaccinated and unvaccinated groups
The associations of vaccination status with conspiracy mentality and beliefs, perceived coercion and polarization are shown in Online Supplemental materials Table S2. We found that both conspiracy mentality and conspiracy beliefs were significantly higher among the unvaccinated rather than the vaccinated group in the US, the UK and China (Figure S1 A and Figure S1 C in the Online Supplemental materials). As pre-registered (Hypotheses 1a and 1b), across cultures the unvaccinated group perceived higher vaccination coercion than the vaccinated group (Figure S1 B in Online Supplemental Material). Within cultures, both unvaccinated and vaccinated groups perceived high levels of vaccination coercion in the US and the UK (i.e. participants scored higher than the average value of 4 on a 7-point scale), but not in China. Contrary to our pre-registered Hypothesis 3, the vaccinated group was more polarized toward unvaccinated people than the unvaccinated group was toward vaccinated people in all three countries (Figure S1 D in Online Supplemental material).
We plotted effect size Cohen’s d and the 95% CI (calculated with the spreadsheet developed by ; see https://osf.io/ixGcd/) in a forest plot (using the R package “forestplot”; ). The forest plot (Figure 1) shows a cross-culturally consistent effect, in that unvaccinated groups scored higher than vaccinated groups on conspiracy mentality, conspiracy beliefs and perceived vaccination coercion. With respect to conspiracy mentality and conspiracy beliefs, the effect of vaccination status appeared smaller in China than in the US and the UK. Interestingly, the effect of vaccination status on polarization was largest in China.
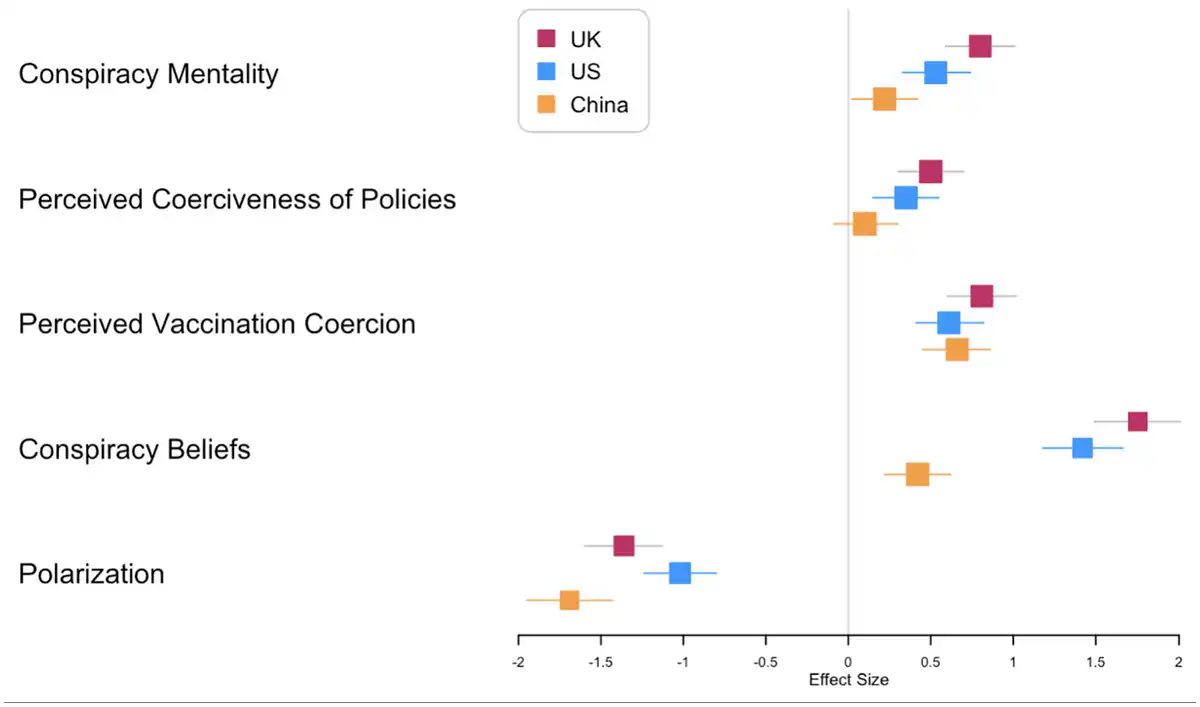
Figure 1
Effect sizes of the differences between the vaccinated and unvaccinated groups.
Effect sizes are Cohen’s d. Effect size larger than 0 means that the unvaccinated group scored higher on a particular dependent variable, while an effect size smaller than 0 means that the vaccinated group scored higher.
Correlation analysis
A correlation analysis (Table S3 in Online Supplemental material) showed that both perceived vaccination coercion and perceived coerciveness of policies were positively correlated with conspiracy mentality and conspiracy beliefs, regardless of vaccination status. Thus, pre-registered Hypothesis 2 was supported. Polarization was positively correlated with perceived vaccination coercion among unvaccinated people, r = 0.25, p < 0.001, while it was negatively correlated with perceived vaccination coercion among vaccinated people, r = −0.21, p < 0.001. The correlations between polarization and conspiracy beliefs were also different between vaccinated and unvaccinated people: It was positive among unvaccinated people, r = 0.47, p < 0.001, and negative among vaccinated people, r = −0.57, p < 0.001.
Moderated mediation analysis
We first conducted a path analysis in each country to determine which paths are moderated by vaccination status (see Online Supplemental materials Table S4). We found moderated mediation effects in all three countries, however, there were differences in terms of the specific paths. Vaccination status moderated only the indirect effect in the US and the UK, but it moderated both the direct and indirect effects in China. These differences notwithstanding, our findings support the pre-registered hypothesis that the effect of perceived vaccination coercion on polarization was mediated by conspiracy beliefs, and this mediation was moderated by vaccination status. More precisely, there was a positive mediation effect among unvaccinated people in all three countries, while this mediation effect was negative among vaccinated people in the US but not in China and the UK (Figure 2).
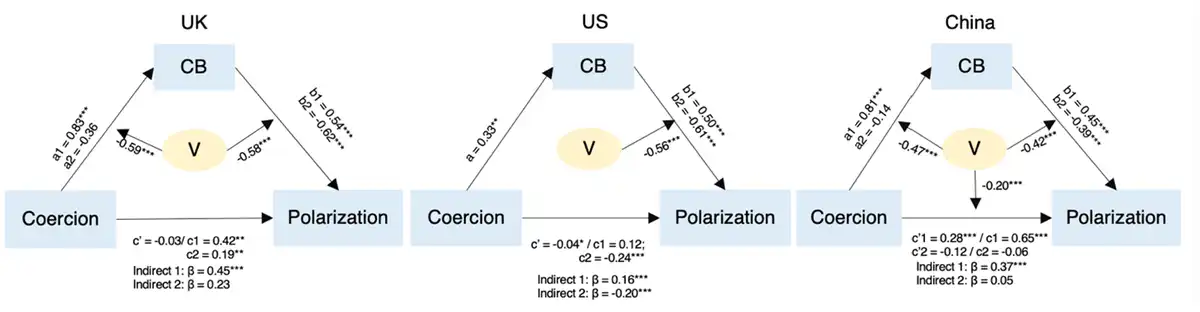
Figure 2
The effect of perceived vaccination coercion on polarization moderated by vaccination status.
Coercion: perceived vaccination coercion; CB: conspiracy beliefs; V: vaccination status. All coefficients are β. Parameters for unvaccinated people are: a1, b1, c1, c’1, and indirect 1; parameters for vaccinated people are: a2, b2, c2, c’2, and indirect 2.
In the US, perceived vaccination coercion predicted conspiracy beliefs (path a in the mediation model), but this effect was not moderated by vaccination status. However, this path was moderated by vaccination status in the UK and China: Perceived vaccination coercion positively predicted conspiracy beliefs among unvaccinated people, while this effect was not significant among vaccinated people (Table S5 in Online Supplemental material). These results indicate that in the US, perceiving stronger vaccination coercion predicts increased conspiracy beliefs regardless of participants’ vaccination status, whereas in the UK and China this effect only emerges among unvaccinated people.
In all three countries, conspiracy beliefs predicted polarization against the opposite vaccination status group (path b in the mediation model), and this effect was moderated by vaccination status. These results suggest that cross-culturally, conspiracy beliefs predict increased polarization among unvaccinated people; interestingly, disbelief in conspiracy theories predicts increased polarization among vaccinated people.
Perceived coerciveness of policies
In a more exploratory fashion, we also conducted a 3 (Country: US; UK; China) × 2 (Vaccination Status: Vaccinated; Unvaccinated) ANOVA (Welch’s) analysis on people’s perceived coerciveness of a range of standardized policies. A main effect of country indicated that people differed in the extent to which they considered a range of prespecified policies coercive in the three countries, F(2, 1198) = 21.62, p < 0.001, ω2 = 0.02. The main effect of vaccination status was significant as well, F (1, 1198) = 27.77, p < 0.001, ω2 = 0.03. We then conducted post-hoc comparisons between countries (see Online Supplemental materials Table S6) and found that the perceived coerciveness of policies was significantly lower in China as compared to the UK and the US; however, there was no difference between the UK and the US. The effects of vaccination status on perceived coerciveness of policies across the three countries were different (Figure 1): Perceived coerciveness of policies was higher among unvaccinated than vaccinated people in the UK and the US, but not in China.
Discussion
This study investigated the effects of vaccination status cross-culturally. Hypotheses 1a, 1b, and 2 were supported as preregistered. Hypothesis 3 was not supported, however, and results in fact revealed the opposite (vaccinated people were more polarized toward unvaccinated people than vice versa). We also tested the mediating role of conspiracy beliefs in the link between perceived vaccination coercion and polarization among vaccinated versus unvaccinated people. While there were some unexpected differences between countries, in all three countries the moderated mediation model analysis revealed that perceived vaccination coercion predicts increased belief in vaccination conspiracy theories; these conspiracy beliefs, in turn, are associated with increased polarization among unvaccinated people. These findings support Hypothesis 4.
The mediation model indicates that conspiracy beliefs play a crucial role in the polarization of unvaccinated people as a function of perceived coercion to get vaccinated. For vaccinated people, perceived vaccination coercion was unrelated to polarization. Moreover, conspiracy beliefs predicted reduced polarization among vaccinated people. This latter finding may suggest that the more strongly vaccinated people reject conspiracy theories, the more strongly they also reject unvaccinated people. However, this mediation model among vaccinated people is less robust than for unvaccinated people, as it fits only in the US, but not in the UK and China.
A notable finding of this study is that vaccinated people were more polarized than unvaccinated people, contradicting Hypothesis 3. Although unexpected, this finding is consistent with an earlier finding that people with low levels of COVID-19 conspiracy beliefs are more likely to end contact with conspiracy believers rather than vice versa (). Similarly, found that vaccinated people have stronger discriminatory attitudes toward unvaccinated people than vice versa. Also, cognitive dissonance could be a factor as people may justify their decision of not being vaccinated to be reasonable. This may have decreased levels of polarization among the unvaccinated.
In an exploratory fashion, we distinguished between perceived vaccination coercion in real life and perceived coerciveness of policies, in consideration of cultural differences in health-related policy perceptions (; ). We specifically sought to consider that (a) within a culture people may differ in how coercive they experience the same set of measures but also that (b) different countries may have different policies. As it turned out, the Chinese sample perceived less vaccination coercion than the UK and the US samples, but that does not mean the measures were less strict in China: Also perceived coerciveness of policies (i.e. participants’ ratings of how coercive a standardized set of policies were independent of whether they were implemented or not) was much lower in China than in the UK and the US. Although speculative, this difference might be explained by the “tightness versus looseness” cultural dimension: Being a typical “tight” culture, China has stricter social norms and punishments (), and this may lead people to be relatively tolerant of strict governmental policies. Another explanation might be that the Chinese had a relatively high acceptance of COVID-19 vaccines (), implying lower levels of perceived coercion. These findings are noteworthy also for policymakers, as they might imply that some measures to stimulate vaccination may work better in some countries than others.
It is important to note that unvaccinated people are not necessarily “anti-vaxxers.” For example, some people might have decided not to be vaccinated for medical reasons. People may have different motives for accepting or refusing vaccination, and therefore we have avoided overinterpretations about people’s underlying motives based on their vaccination status.
Implications
The risks of a COVID-19 infection differ across people; for example, elderly people are more likely to have life-threatening symptoms when they are infected. The COVID-19 pandemic therefore has created a complex situation in which governments had to deal with a multi-level social dilemma between collective versus individual interests (). Many countries have resorted to policies which could be construed as coercive, but that are likely to have increased vaccination uptake. Our findings suggest that these measures also may have had a downside, as they predict conspiracy beliefs and polarization especially among unvaccinated people. This is likely to have downstream implications for public health. found that believing in COVID-19 vaccine conspiracies were related to reduced trust in science and official information. In the vaccination campaign, more objective arguments other than moral persuasion strategies therefore should be applied to reduce societal polarization (). To increase the uptake of vaccination rate, people need easy access not only to the vaccine, but also to trustworthy information that prebunks and debunks conspiracy theories (). For example, people should be encouraged to discuss COVID-19 vaccines with their healthcare provider when they are hesitant about vaccination, given that people generally perceive healthcare providers as more trustworthy than politicians (). In addition, scientific communication about vaccination safety is more effective in overcoming hesitancy than imposing coercive policies ().
Strengths and limitations
This study has various strengths and limitations. Among the strengths are that we collected data in three countries, including a non-WEIRD society (China). Indeed, there were cultural differences for some of the results in this study, especially China as compared with the US and UK. This suggests that in future research, more cross-cultural studies about the link between conspiracy beliefs and health behavior are needed. Furthermore, although we present only one study, it had a strong methodology: We preregistered this study, conducted it in three different countries, and it was well-powered with a big sample size. These methodological features suggest that the results are reliable. Finally, by contrasting people with a different vaccination status, this study offers clear relevance for public health and the consequences of public health policies.
There are also noteworthy limitations of this study. One issue is that the samples in each country were not representative for their population. For example, elderly and sick people who benefited tremendously from the vaccine were underrepresented. Also, the reliability of the conspiracy belief measures is different across the three countries, which suggests that conspiracy beliefs may be to some degree culture specific; moreover, we should highlight that the conspiracy belief measure consisted of self-designed items. It is important to acknowledge the possibility that cultural differences, or differences in policies between nations, can influence the nature of the conspiracy theories, and therefore the specific meaning of the items. Moreover, this is a cross-sectional study, and hence does not show the causality of the relations investigated here. This makes it also difficult to control for common method variance, which may inflate the effect sizes.
In addition, polarization is a complex construct, and it is difficult to capture the nature of polarization in one single measure. As polarization is often domain-specific, precise measurements are always a challenge in this research area. Moreover, we used a single item to measure perceived vaccination coercion, and future research would benefit from more items that complement each other (e.g. by tapping various forms of coercion that people may perceive). Finally, our study focused on understanding polarization among unvaccinated people; however, our results suggested that vaccinated people are more polarized toward unvaccinated people than vice versa. More research is needed to explain and replicate this finding, also in the aftermath of the COVID-19 pandemic.
Concluding remarks
Perceived vaccination coercion is associated with increased vaccination-related conspiracy beliefs and polarization among unvaccinated people. The current findings suggest that policy makers faced a trade-off between public health and social cohesion during the COVID-19 pandemic. Both the benefits and drawbacks of potentially coercive vaccination measures should be considered in decision-making around this precarious issue. Not only the coronavirus, but also health-related conspiracy theories are harmful to public health and might damage social cohesion. Therefore, vaccination policies should be implemented carefully, to reduce the risk of replacing an epidemic for an infodemic.
Author contributions Haiyan Wang: conceptualization, data curation, formal analysis, investigation, methodology, project administration, writing – original draft preparation, writing – review and editing. Jan-Willem van Prooijen: conceptualization, supervision, writing – review and editing. Paul A.M. van Lange: conceptualization, supervision, writing – review and editing.
Data sharing statement The datasets generated during and/or analyzed during the current study are available in OSF at https://osf.io/gqj2s/.
Declaration of conflicting interests The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the China Scholarship Council [grant number 201907070011].
Ethics approval The authors assert that all procedures contributing to this work comply with the ethical standards of Scientific and Ethical Review Board (VCWE) of the Faculty of Behavioural and Movement Sciences at Vrije Universiteit Amsterdam, approval number: VCWE-S-21-00228[80].
Informed consent All participants provided informed consent before participating in this study.
Pre-registration This study was pre-registered in OSF at https://osf.io/4bcd8, all pre-registered hypotheses were reported in the manuscript.
Supplemental material Supplemental material for this article is available online.
Haiyan Wang
https://orcid.org/0000-0001-6052-4736
Jan-Willem van Prooijen
https://orcid.org/0000-0001-6236-0819
1. Note that Hypotheses 3 and 4 in the paper are listed as Hypotheses 1c and 3 in the pre-registration.
References
- Abeywickrama RS, Rhee JJ, Crone DL, et al. (2020) Why moral advocacy leads to polarization and proselytization: The role of self-persuasion. Journal of Social and Political Psychology 8(2): 473–503.
- Ajzen I (1991) The theory of planned behavior. Organizational Behavior and Human Decision Processes 50(2): 179–211.
- Allington D, Duffy B, Wessely S, et al. (2021) Health-protective behaviour, social media usage and conspiracy belief during the COVID-19 public health emergency. Psychological Medicine 51(10): 1763–1769.
- Aronson E (1969) The theory of cognitive dissonance: A current Perspective this article and all the original work reported in it were supported by a grant from the National Science Foundation. In: Berkowitz L (ed.) Advances in Experimental Social Psychology. New York and London: Academic Press, pp.1–34. Available at: https://www.sciencedirect.com/science/article/pii/S0065260108600751 (accessed 7 November 2022).
- Bacon AM, Taylor S (2021) Vaccination hesitancy and conspiracy beliefs in the uk during the sars-cov-2 (covid-19) pandemic. International Journal of Behavioral Medicine 29: 448–455.
- Bardosh K, de Figueiredo A, Gur-Arie R, et al. (2022) The unintended consequences of COVID-19 vaccine policy: why mandates, passports and restrictions may cause more harm than good. BMJ Global Health 7(5): e008684.
- Van Bavel JJ, Baicker K, Boggio PS, et al. (2020) Using social and behavioural science to support COVID-19 pandemic response. Nature Human Behaviour 4(5): 460–471.
- Bernerth JB, Aguinis H (2016) A Critical Review and Best-practice recommendations for control variable usage. Personnel Psychology 69(1): 229–283.
- Bielski Z (2021) For half-vaccinated couples, the relationship status is doubly complicated. The Globe and Mail, . Available at: https://www.theglobeandmail.com/canada/article-for-half-vaccinated-couples-the-relationship-status-is-doubly/ (accessed 28 March 2022).
- Bierwiaczonek K, Kunst JR, Pich O (2020) Belief in COVID-19 conspiracy theories reduces social distancing over time. Applied Psychology. Health and Well-Being 12(4): 1270–1285.
- Bor A, Jørgensen F, Petersen MB (2023) Discriminatory attitudes against unvaccinated people during the pandemic. Nature 613: 704–711.
- Bruder M, Haffke P, Neave N, et al. (2013) Measuring individual differences in generic beliefs in conspiracy theories across cultures: Conspiracy Mentality Questionnaire. Frontiers in Psychology 4: 43078.
- Choi D, Chun S, Oh H, et al. (2020) Rumor propagation is amplified by echo chambers in social media. Scientific Reports 10(1): 310.
- Cinelli M, De Francisci Morales G, Galeazzi A, et al. (2021) The echo chamber effect on social media. Proceedings of the National Academy of Sciences 118(9): e2023301118.
- Del Vicario M, Vivaldo G, Bessi A, et al. (2016) Echo chambers: Emotional contagion and group polarization on Facebook. Scientific Reports 6(1): 37825.
- Earnshaw VA, Eaton LA, Kalichman SC, et al. (2020) COVID-19 conspiracy beliefs, health behaviors, and policy support. Translational Behavioral Medicine 10(4): 850–856.
- Ellyatt H (2021) As many return to the office, tensions flare between the ‘vaxxed and unvaxxed’. Available at: https://www.cnbc.com/2021/09/13/office-tensions-rise-between-the-vaccinated-and-unvaccinated-.html (accessed 28 March 2022).
- Enders AM, Smallpage SM (2019) Informational cues, partisan-motivated reasoning, and the manipulation of conspiracy beliefs. Political Communication 36(1): 83–102.
- Festinger L (1957) A Theory of Cognitive Dissonance. Stanford: Stanford University Press.
- Freeman D, Waite F, Rosebrock L, et al. (2022) Coronavirus conspiracy beliefs, mistrust, and compliance with government guidelines in England. Psychological Medicine 52: 251–263.
- Garry J, Ford R, Johns R (2022) Coronavirus conspiracy beliefs, mistrust, and compliance: Taking measurement seriously. Psychological Medicine 52: 3116–3126.
- Gelfand MJ, Raver JL, Nishii L, et al. (2011) Differences between tight and loose cultures: A 33-Nation Study. Science 332(6033): 1100–1104.
- Gordon M, Lumley T (2021) Advanced forest plot using ‘grid’ graphics. Available at: https://cran.r-project.org/web/packages/forestplot/forestplot.pdf (accessed 26 January 2022).
- Hagen L, Fox A, O’Leary H, et al. (2021) Polarization of COVID-19 vaccine discourse on Twitter: Implications for vaccine policy. JMIR Infodemiology, . Available at: http://preprints.jmir.org/preprint/34231 (accessed 23 February 2022).
- Hammer C, Cristea V, Dub T, et al. (2021) High but slightly declining COVID-19 vaccine acceptance and reasons for vaccine acceptance, Finland April to December 2020. Epidemiology and Infection 149: e123.
- Henkel L, Sprengholz P, Korn L, et al. (2022) The association between vaccination status identification and societal polarization. Nature Human Behaviour 7: 231–239.
- Howard MC, Davis MM (2023) The mediating role of vaccine hesitancy in the relations of COVID-19 conspiracy beliefs and vaccination outcomes: Which dimensions matter? Journal of Health Psychology 28(3): 241–250.
- Imhoff R, Lamberty P (2020) A bioweapon or a hoax? The link between distinct conspiracy beliefs about the coronavirus disease (COVID-19) outbreak and pandemic behavior. Social Psychological and Personality Science 11(8): 1110–1118.
- Imhoff R, Bertlich T, Frenken M (2022) Tearing apart the “evil” twins: A general conspiracy mentality is not the same as specific conspiracy beliefs. Current Opinion in Psychology 46: 101349.
- Jamovi (Version 1.6) (2021) Available at: https://www.jamovi.org (accessed 18 January 2022).
- Jensen EA, Pfleger A, Herbig L, et al. (2021) What drives belief in vaccination conspiracy theories in Germany? Frontiers in Communication 6: 678335.
- Jost JT, Baldassarri DS, Druckman JN (2022) Cognitive–motivational mechanisms of political polarization in social-communicative contexts. Nature Reviews Psychology 1(10): 560–576.
- Jovančević A, Milićević N (2020) Optimism-pessimism, conspiracy theories and general trust as factors contributing to COVID-19 related behavior – A cross-cultural study. Personality and Individual Differences 167: 110216.
- Kofta M, Soral W, Bilewicz M (2020) What breeds conspiracy antisemitism? The role of political uncontrollability and uncertainty in the belief in Jewish conspiracy. Journal of Personality and Social Psychology 118(5): 900–918.
- Kossowska M, Bukowski M (2015) Motivated roots of conspiracies: The role of certainty and control motives in conspiracy thinking. In: Bilewicz M, Cichocka A, Soral W (eds) The Psychology of Conspiracy. New York, NY: Routledge/Taylor & Francis Group, pp.145–161. Available at: https://search.ebscohost.com/login.aspx?direct=true&db=psyh&AN=2015-33221-008&site=ehost-live.
- Kunda Z (1990) The case for motivated reasoning. Psychological Bulletin 108(3): 480–498.
- Lakens D (2013) Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Frontiers in Psychology 4: 863.
- Lazarus JV, Ratzan SC, Palayew A, et al. (2021) A global survey of potential acceptance of a COVID-19 vaccine. Natural Medicines 27(2): 225–228.
- MacDonald N, Dubé, Comeau J (2022) Vaccines, politics and mandates: Can We see the forest for the trees? International Journal of Health Policy and Management 12: 7572.
- Mathieu E, Ritchie H, Rodés-Guirao L, et al. (2020) Coronavirus Pandemic (COVID-19). Our World in Data. Available at: https://ourworldindata.org/coronavirus (accessed 25 November 2021).
- Meissner D (2021) ‘Irresponsible and selfish;’ New poll finds rising tension between vaccinated and unvaccinated Canadians. Available at: https://www.cp24.com/news/irresponsible-and-selfish-new-poll-finds-rising-tension-between-vaccinated-and-unvaccinated-canadians-1.5601596?cache=yes%3Fot%3DAjaxLayout%3FclipId%3D64268%3FcontactForm%3Dtrue (accessed 28 March 2022).
- Mello MM, Opel DJ, Benjamin RM, et al. (2022) Effectiveness of vaccination mandates in improving uptake of COVID-19 vaccines in the USA. Lancet 400(10351): 535–538.
- Middleman AB, Klein J, Quinn J (2021) Vaccine hesitancy in the time of COVID-19: Attitudes and intentions of teens and parents regarding the COVID-19 vaccine. Vaccines 10(1): 4.
- Miller JM, Saunders KL, Farhart CE (2016) Conspiracy endorsement as motivated reasoning: The moderating roles of Political Knowledge and Trust. American Journal of Political Science 60(4): 824–844.
- Nast C (2021) In schools, tensions between vaccinated and unvaccinated students rise. Available at: https://www.teenvogue.com/story/vaccination-status-in-schools-is-causing-tension-among-students (accessed 28 March 2022).
- Peer E, Rothschild D, Gordon A, et al. (2022) Data quality of platforms and panels for online behavioral research. Behavior Research Methods 54(4): 1643–1662.
- Van Prooijen J-W (2022) Psychological benefits of believing conspiracy theories. Current Opinion in Psychology 47: 101352.
- Romer D, Jamieson KH (2020) Conspiracy theories as barriers to controlling the spread of COVID-19 in the US. Social Science & Medicine 263: 113356.
- Rosseel Y (2012) Lavaan: An R package for structural equation modeling. Journal of Statistical Software 48(2): 1–36.
- Ruiz JB, Bell RA (2021) Predictors of intention to vaccinate against COVID-19: Results of a nationwide survey. Vaccine 39(7): 1080–1086.
- Sabat I, Neuman-Böhme S, Varghese NE, et al. (2020) United but divided: Policy responses and people’s perceptions in the EU during the COVID-19 outbreak. Health Policy 124(9): 909–918.
- Schmidt AL, Zollo F, Scala A, et al. (2018) Polarization of the vaccination debate on Facebook. Vaccine 36(25): 3606–3612.
- Schuessler J, Dinesen PT, Østergaard SD, et al. (2022) Public support for unequal treatment of unvaccinated citizens: Evidence from Denmark. Social Science & Medicine 305: 115101.
- Sheng H, Feng T, Liu L (2023) The influence of digital transformation on low-carbon operations management practices and performance: Does CEO ambivalence matter? International Journal of Production Research 61(18): 6215–6229.
- Sparks G, Lopes L, Montero A, et al. (2022) KFF COVID-19 vaccine monitor: April 2022. KFF. Available at: https://www.kff.org/coronavirus-covid-19/poll-finding/kff-covid-19-vaccine-monitor-april-2022/ (accessed 16 November 2023).
- Stojanov A, Halberstadt J (2020) Does lack of control lead to conspiracy beliefs? A meta-analysis. European Journal of Social Psychology 50: 955–968.
- Stojanov A, Halberstadt J, Bering JM, et al. (2023) Examining a domain-specific link between perceived control and conspiracy beliefs: A brief report in the context of covid-19. Current Psychology 42: 6347–6356.
- Van der Linden S (2022) Misinformation: Susceptibility, spread, and interventions to immunize the public. Natural Medicines 28: 460–467.
- Van Lange PAM, Rand DG (2022) Human cooperation and the crises of climate change, COVID-19, and misinformation. Annual Review of Psychology 73: 379–402.
- Van Prooijen J-W, Acker M (2015) The influence of control on belief in conspiracy theories: Conceptual and applied extensions. Applied Cognitive Psychology 29(5): 753–761.
- Van Prooijen J-W (ed.) (2021) The Psychology of Political Polarization (Current issues in social psychology). Abingdon, Oxon; New York, NY: Routledge.
- Van Prooijen J-W, Amodio DM, Boot A, et al. (2023a) A longitudinal analysis of conspiracy beliefs and Covid-19 health responses. Psychological Medicine 53: 5709–5716.
- Van Prooijen J-W, Böhm N (2023) Do conspiracy theories shape or rationalize vaccination hesitancy over time? Social Psychological and Personality Science 15(4): 421–429.
- Van Prooijen J-W, Etienne TW, Kutiyski Y, et al. (2023b) Conspiracy beliefs prospectively predict health behavior and well-being during a pandemic. Psychological Medicine 53: 2514–2521.
- Van Prooijen J-W, Van Lange PAM (2014) The social dimension of belief in conspiracy theories. In: Van Prooijen J-W, Van Lange PAM (eds) Power, Politics, and Paranoia: Why People Are Suspicious of Their Leaders. Cambridge: Cambridge University Press, pp.237–253. Available at: https://www.cambridge.org/core/books/power-politics-and-paranoia/social-dimension-of-belief-in-conspiracy-theories/3EA14FDA1702A109657E755F848457C1 (accessed 20 April 2021).
- Von Lengerke T, Vinck J, Rütten A, et al. (2004) Health policy perception and health behaviours: A multilevel analysis and implications for public health psychology. Journal of Health Psychology 9(1): 157–175.
- Wang H, Van Prooijen J-W (2023) Stolen elections: How conspiracy beliefs during the 2020 American presidential elections changed over time. Applied Cognitive Psychology 37(2): 277–289.
- Winter K, Pummerer L, Hornsey MJ, et al. (2022) Pro-vaccination subjective norms moderate the relationship between conspiracy mentality and vaccination intentions. British Journal of Health Psychology 27: 390–405.
- Zarocostas J (2020) How to fight an infodemic. Lancet 395(10225): 676.